History
Pt came into the ED last month for RLQ pain and was diagnosed with appendicitis due to cecal mass. He was scheduled for R hemicolectomy which was deferred on the day of surgery due to worsening AKI. Pt has returned for R hemicolectomy at this point. Pre-op labs were significant for hyperkalemia and elevated BUN and creatinine, but was cleared for surgery.
S
63 year old male POD 1 s/p R hemicolectomy for cecal mass, which was sent for biopsy. There were no acute events overnight. Pt is on a PCA. Pt was seen and examined at bedside. Pt’s pain is well controlled and is in no acute distress. Pt has been voiding appropriately. Pt denies nausea, vomiting, bowel movements and passing gas.
O
Vital signs
- BP: 167/91 (range- 123/73 to 177/96)
- HR: 85 bpm regular rate, rhythm and amplitude (range- 83 to 94)
- RR: 19/min regular rate and rhythm, unlabored (range- 8 to 19)
- Temp: 37 C, orally
I/Os
- Urine: 1700/2035 pale yellow urine
- JP drain: 20/70 serosanguinous fluid
Physical exam
- General: Well developed, well nourished male in no apparent discomfort. Appears stated age of 63. Alert and oriented x3.
- Lungs: Unlabored breathing, clear to auscultation bilaterally. No adventitious sounds.
- Heart: Regular rate and rhythm.
- Abdomen: Abdomen soft, non-distended, flat and symmetric with no striae or pulsations noted. No tenderness, guarding or rebound noted. Incision sites healing well- clean and dry, no signs of infection (erythema, warmths, exudates).
- Extremities: No erythema, warmth or crepitus noted. No pitting edema noted. Non-tender to palpation. Full range of motion of all upper and lower extremities bilaterally.
- Neuro: Sensation is intact bilaterally to pain and light touch. Good muscle tone.
Labs
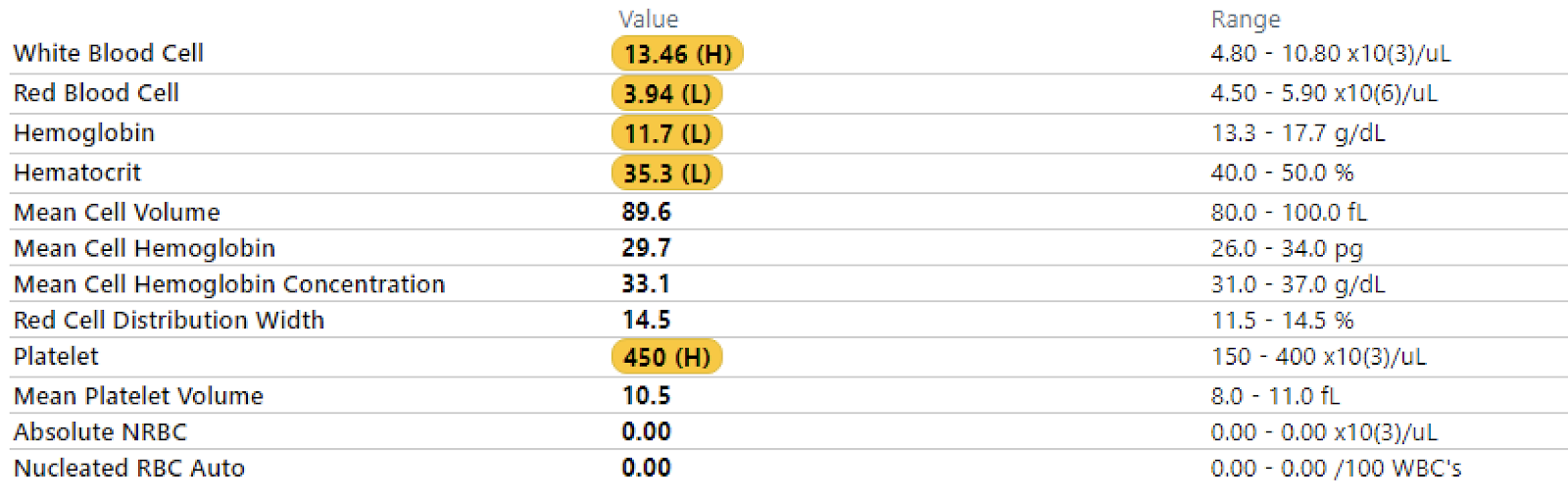
- CBC
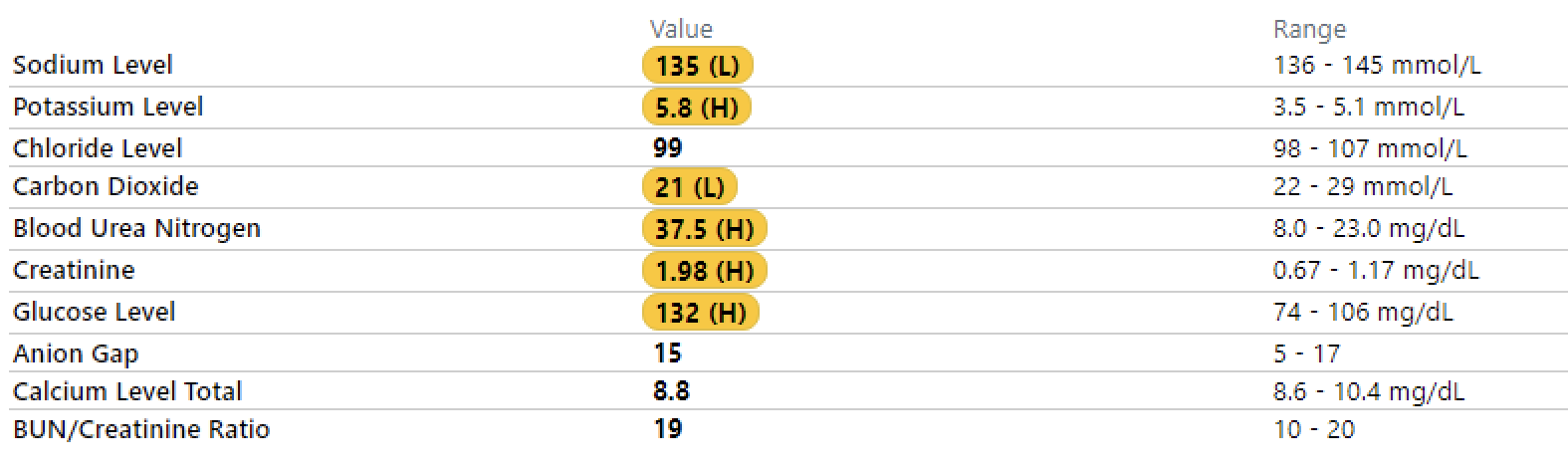
- BMP
A
63 year old male POD 1 s/p laparoscopic right hemicolectomy. Pt tolerated the procedure well and is having adequate pain control. Vitals remain within normal limits. Pt had known elevated BUN and creatinine and hyperkalemia pre-operatively which persists post-op. Creatine is coming down appropriately while hyperkalemia is persisting. Pt has mild anemia which is to be expected following the procedure. All other labs are unremarkable. There is nothing of note on physical exam.
P
- Post-op
- Morning labs (CBC, BMP)
- Remove foley
- Maintain clear liquid diet
- Continue PCA for pain control
- Continue Entereg 12 mg PO Q12H
- Nutrition consult
- PT
- DVT prophylaxis
- Lovenox 40 mg subq Q24H
- Elevated creatinine
- IV fluids- sodium chloride, 100 mL/hr
- Hyperkalemia
- Calcium gluconate 1 g in sodium chloride 0.675% IV one time over 30 minutes
- Insulin Lispro 10 U IV over 0.5 minutes