History
71 year old male presented to ED 3 days ago complaining of RLQ pain x4 days. A CTAP was done which showed an inseparable cystic focus at the base of the cecum. They said it was likely to be an inflamed mucocele, however malignancy could not be excluded. They felt it was less likely to be acute appendicitis. The surgical team was consulted and pt was admitted to our care. Over the course of his stay, pt had slight elevation of WBC (~14) but otherwise pt remained stable. Pt received bowel prep, with no adverse reactions, last night for his colonoscopy today.
S
71 year old male hospital day 3 with complaints of RLQ pain. There were no acute events overnight. Pt was seen and examined at bedside after returning from his colonoscopy. Pt mentions that his RLQ pain is improving, however says that the pain is still present. Pt says that his last bowel movement was early this morning. All bowel movements from last night were non-bloody. Pt has been passing gas throughout the day. Pt admits to urinating once since returning from the colonoscopy. Pt denies hematuria, dysuria, nausea, vomiting and pain anywhere else in his body.
O
Vital signs
- BP: 164/87 (range- 83/58 to 164/87)
- 83/58 likely due to pressure dropping with sedation during the colonoscopy
- HR: 72 bpm regular rate, rhythm and amplitude (range- 55 to 89)
- RR: 18/min regular rate and rhythm, unlabored (range- 12-22)
- Temp: 36.1 C, orally
Physical exam
- General: Well developed, well nourished male in no apparent discomfort. Appears stated age of 71. Alert and oriented x3.
- Lungs: Unlabored breathing, clear to auscultation and percussion bilaterally. No adventitious sounds.
- Heart: Regular rate and rhythm.
- Abdomen: Abdomen flat and symmetric with no scars, striae or pulsations noted. Bowel sounds normoactive in all 4 quadrants with no aortic/renal/iliac or femoral bruits. Moderate tenderness to palpation of the RLQ. Mild fullness of bilateral lower abdomen. No guarding or rebound noted. No CVA tenderness noted.
- Extremities: No erythema, warmth or crepitus noted. No pitting edema noted. Non-tender to palpation. Full range of motion of all upper and lower extremities bilaterally.
- Neuro: Sensation is intact bilaterally to pain and light touch. Good muscle tone.
Labs/imaging
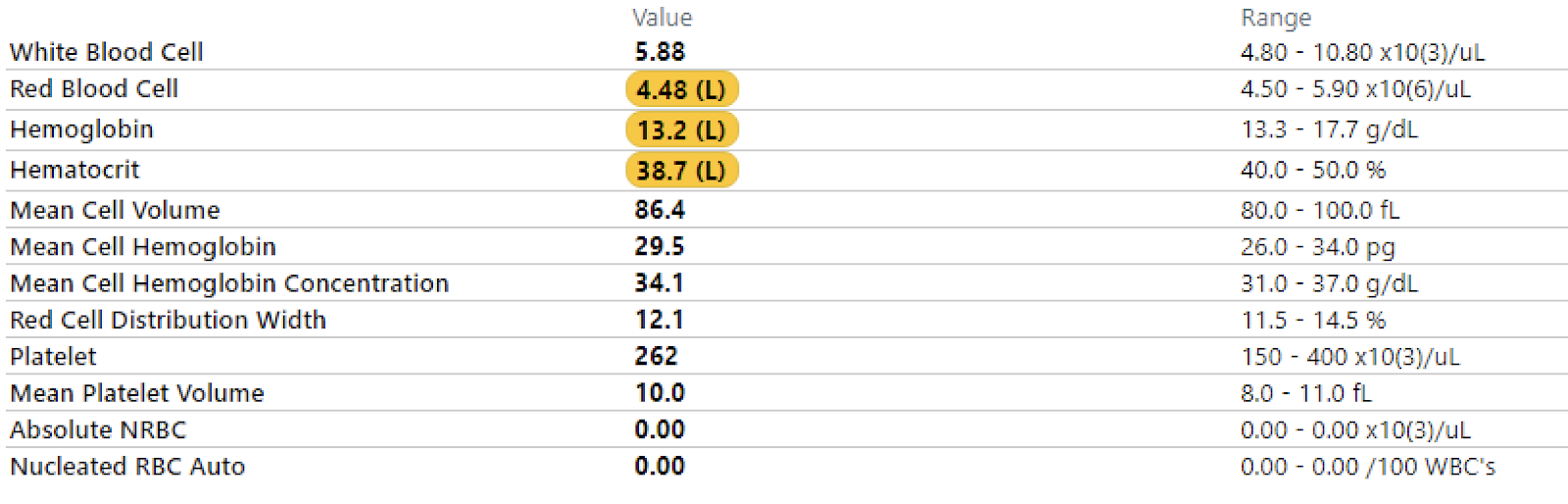
- CBC
- BMP
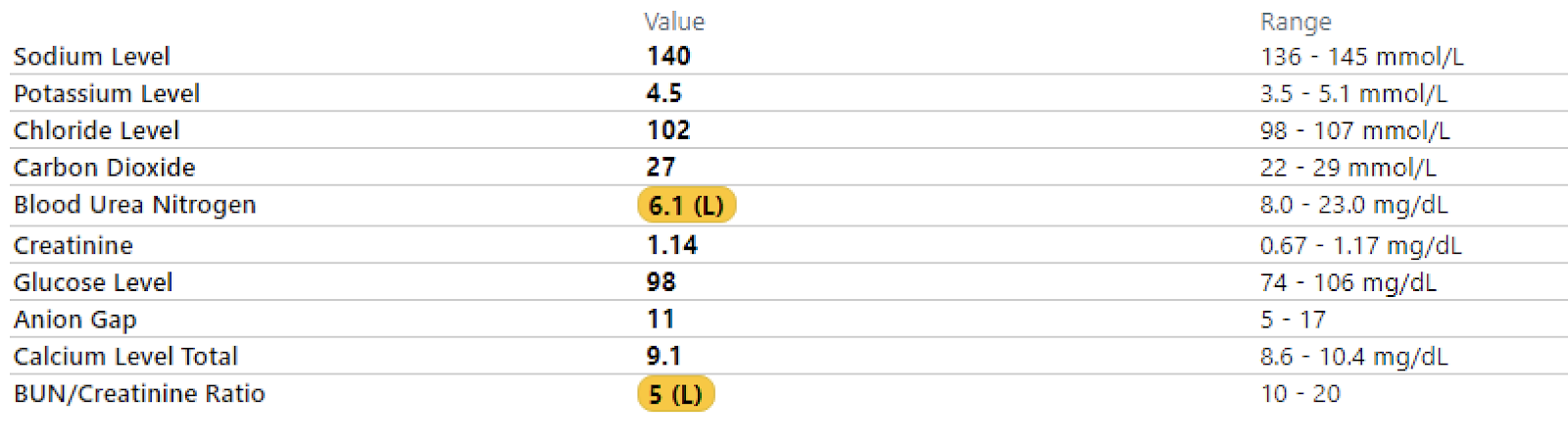
- Electrolytes


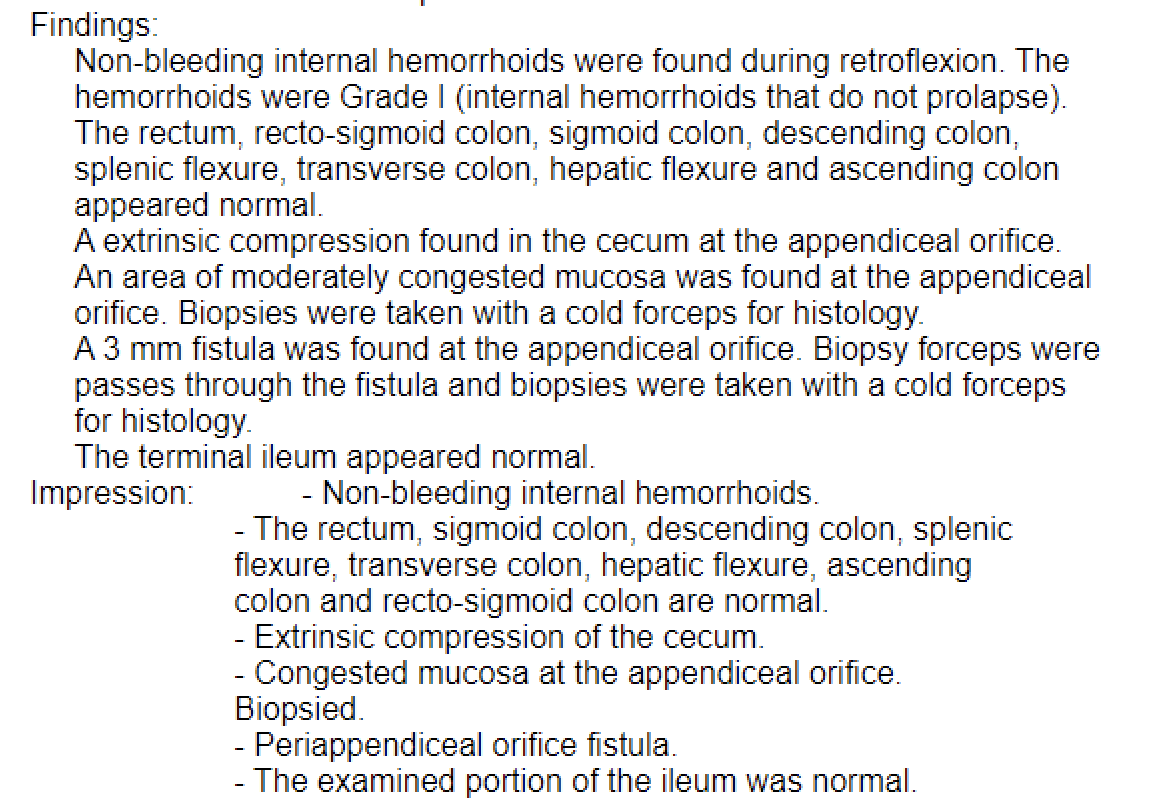
- Colonoscopy
A
71 year old male hospital day 3 for RLQ pain in stable condition. Pain is subjectively improving and labs and vitals remain within normal limits. BUN is low, which is likely due to his NPO status as this is a common finding in pts who are NPO. Pt underwent colonoscopy today with results indicating an extrinsic compression of the appendix and a 3 mm fistula of the appendiceal orifice. Biopsies were taken of both areas, with results still pending.
P
- Consider inpatient vs. outpatient elective surgical resection of the mass
- Pain control
- Tylenol 975 mg PO Q6H PRN
- Continue Zosyn 4,500 mg in 100 mL D5W 25 mL/hr Q8H (for the remainder of the course)
- Reduce fluids from 100 mL/hour to 75 mL/hr
- Remain NPO until further decision is made regarding surgery