History
CC:
“My stomach is killing me” x2 days.
HPI:
Pt is a 61 year old female with a pmhx of HTN who presented to the ED late last night with complaints of abdominal pain for the past 2 days. Pt states that the pain is located in the LLQ region with no radiation. She mentions that the pain is sharp in nature and has been constant since the pain began. At its worst, the pain reached 10/10 in severity. She does mention that she had similar episodes of pain over the past few months that were milder in nature and resolved on their own. She does not recall doing anything differently before the painful bouts began. Pt denies trying any medications at home and does not know of anything that made her pain better or worse. Pt admits to associated bloating, subjective chills, nausea and non-bloody non-bilious vomiting. Pt’s states that her most recent colonoscopy was 5 years ago where benign diverticula were observed. LMP was at age 53.
Denies diarrhea, constipation, cough, congestion, sick contacts, recent antibiotic use, hematuria, dysuria, urinary frequency, vaginal discharge, hematemesis, history of ovarian cysts and recent travel.
Today is hospital day 1 and pt says she feels better. She states that her abdomen still feels a little tender but thinks it is just because she needs to heal. She is expressing a desire to go home and says she cannot spend another night here.
Pmhx:
- HTN x unknown years
Home medications:
- Lisinopril 10 mg PO QD for HTN
Hospital medications:
- Ciprofloxacin 400 mg in D5W 200 mL IV x1 dose
- Metronidazole 500 mg in 100 mL fluid IV x1 dose
- Piperacillin/tazobactam 3.375 g in D5W 100 mL IV Q8H
Surgical History:
- No past surgical history.
Allergies:
- No known drug/food/environmental allergies
Family History:
- Unknown
- Known family history of HTN, unknown in who.
- No known family hx cancer, DM, cardiovascular disease
Social History:
- Smoking: Denies
- Alcohol: Denies
- Illicit drug use: Denies
- Marital History: Married
- Language: English
- Occupational History: Unemployed
- Travel: No recent travel
- Home situation: Lives with her husband on long island
- Sleep: Endorses sleeping about 7-8 hours at night and feeling well rested
- Exercise: Maintains an active lifestyle and tries to workout at least a half hour daily.
- Diet: Admits to a healthy diet heavy on fruits, vegetables and lean protein with whole grain carbs.
- Caffeine: Admits to 2 cups of coffee daily.
ROS:
- General: Admits to chills. Denies night sweats, weight loss/gain, fever, fatigue and change in appetite.
- Skin, hair, nails: Denies discolorations, moles, rashes, changes in hair distribution or texture, pruritus.
- HEENT: Denies head trauma, vertigo, visual disturbances, ear pain, hearing loss, tinnitus, epistaxis, discharge, congestion, sore throat, bleeding gums.
- Neck: Denies localized swelling/lumps, stiffness/decreased ROM
- Pulmonary: Denies dyspnea, cough, wheezing, cyanosis and hemoptysis.
- Cardiovascular: Denies palpitations, chest pain and swelling of lower extremities.
- Gastrointestinal: Admits to abdominal pain, nausea, vomiting and bloating. Denies constipation, dysphagia, pyrosis, flatulence, eructation, rectal bleeding, hemorrhoids, blood in stool and diarrhea.
- Genitourinary: Denies urinary frequency, nocturia, dysuria, urgency, flank pain, oliguria, polyuria and incontinence.
- Musculoskeletal: Denies joint pain, joint swelling, back pain, muscle pain and arthritis.
- Nervous system: Denies seizures, headache, loss of consciousness, ataxia, loss of strength, change in cognition/mental status/memory.
- Peripheral vascular: Denies intermittent claudication, coldness or trophic changes, varicose veins, peripheral edema, or color changes.
- Hematologic: Denies anemia, easy bruising or bleeding, lymph node enlargement, history of DVT/PE.
- Endocrine: Denies diaphoresis, polyuria, polydipsia, polyphagia, heat or cold intolerance, goiter or hirsutism.
- Psychiatric: Denies feelings of helplessness, hopelessness, lack of interest in usual activities, or suicidal ideations, anxiety, obsessive/compulsive disorder, aditory/visual/tactile hallucinations or ever seeing a mental health professional.
Physical
General:
- Well developed, well nourished female in no apparent discomfort appears stated age of 61. Neatly groomed, in hospital gown, alert and oriented x4. Ambulates well without support.
Vital Signs:
- BP: 124/82 mm Hg
- R: 18/min, regular rate and rhythm, unlabored
- P: 94 beats per minute, regular rate, rhythm and amplitude
- T: 98.3 degrees F (oral)
- O2 Sat : 96% room air
- Height: 61 inches Weight: 119 lbs BMI: 22.5
Skin & Head:
- Skin: Warm and moist, good turgor. Nonicteric, no lesions, scars, or tattoos noted.
Nose/Sinuses:
- Nose: Symmetrical. No discharge visualized. Nares patent bilaterally. Nasal mucosa is pink and well hydrated. Septum midline without lesions, deformities, injection, or perforation. No foreign bodies.
Thorax and Lungs:
- Chest: Symmetrical, no deformities, no trauma. Respirations unlabored/ no paradoxical respirations or use of accessory muscles noted. Non-tender to palpation throughout.
- Lungs: Clear to auscultation and percussion bilaterally. No adventitious sounds.
Cardiac Exam:
- Regular rate and rhythm. S1 and S2 are distinct with no murmurs, S3 or S4. No splitting of S2 or friction rubs appreciated.
Abdominal Exam:
- Abdomen with flat contour with no scars, striae or pulsations noted. Bowel sounds normoactive in all 4 quadrants with no aortic/renal/iliac or femoral bruits. Mild tenderness diffusely, no guarding or rebound noted. No CVA tenderness.
Mental status exam:
- Patient is well appearing, has good hygiene and is neatly groomed. Patient is alert and oriented to name, date, time and location. Speech and language ability intact, with normal quantity, fluency, and articulation. Patient denies changes to mood. Conversation progresses logically. Insight, judgment, cognition, memory and attention intact.
Differential diagnosis:
- Diverticulitis
- IBD
- Nephrolithiasis
- Ovarian cancer
Labs:
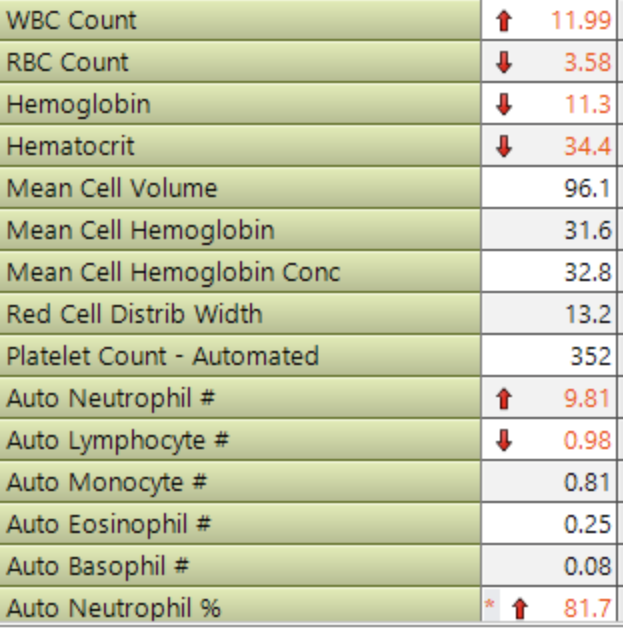
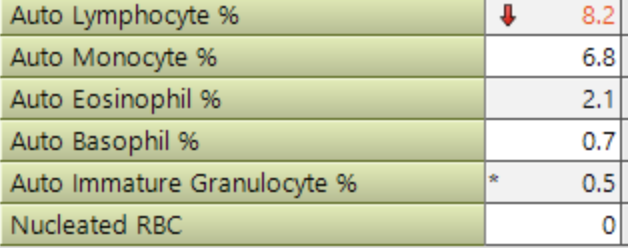
- CBC
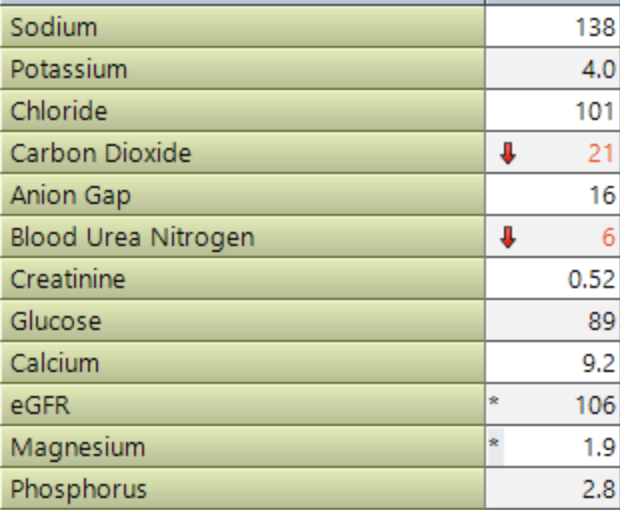
- BMP
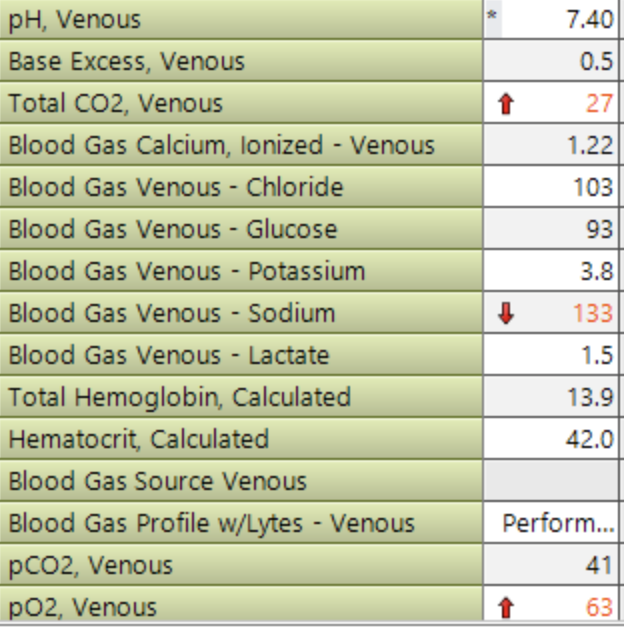
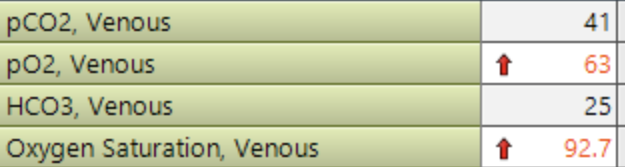
- VBG
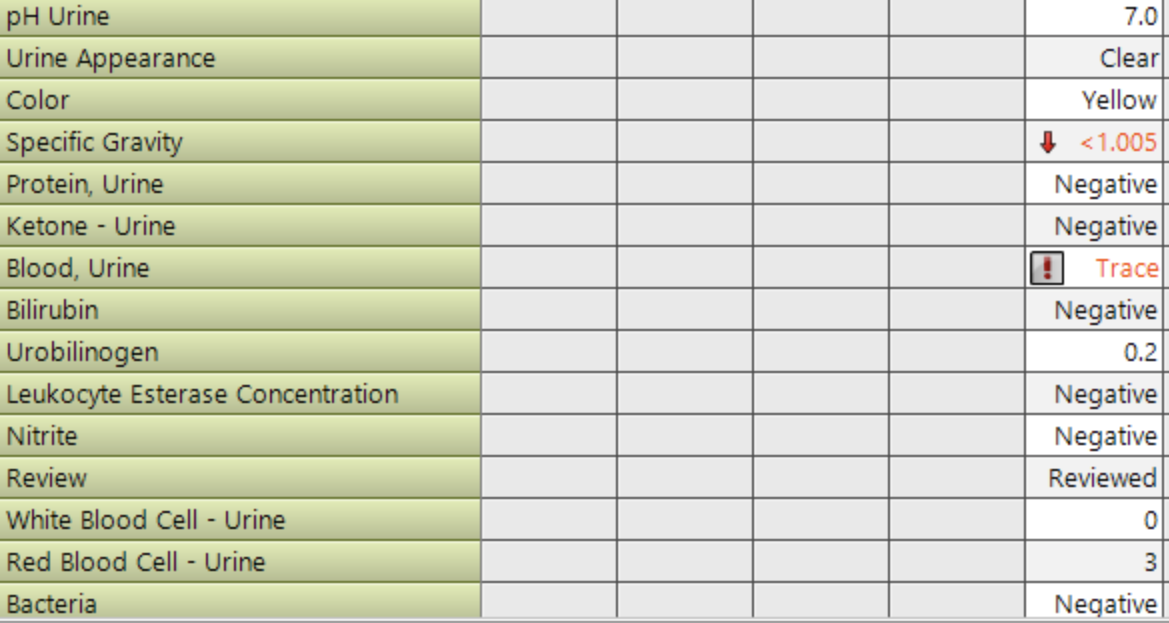
- U/a
Imaging:
- CT abdomen pelvis
- Colonic diverticulosis involving the descending colon and sigmoid. There appears to be a segment of wall thickening of the proximal sigmoid with subtle pericolic fat infiltration suggesting mild acute diverticulitis. No macro perforation. No pericolic abscess.
- EKG
- Normal sinus rhythm
- Chest x-ray
- No pneumoperitoneum.
- Clear lungs.
Assessment:
- 61 year old female who presented to the ED for abdominal pain with associated bloating and vomiting. Imaging in the ED was significant for diverticulitis, without perforation. Pt was started on 1 dose of metronidazole and ciprofloxacin. Pt was then started on piperacillin/tazobactam Q8H. Today is HD #1 and pt says she is subjectively feeling better. Vitals are within normal limits today, and on exam pt displayed mild diffuse abdominal tenderness. Labs are significant for elevated WBC at ~12, which is trending down from yesterdays ~13. Labs also show mild anemia with a hgb of 11.3, likely due to dilutional effects of the IVs she has been receiving. All other labs are unremarkable. At this time, continued initial stabilization should be achieved before discharge.
Diagnosis:
- Diverticulitis
Plan:
- Diverticulitis
- ID consult for PO antibiotic guidance
- Complete 1 more dose of zosyn in hospital
- Advance diet based on toleration- full liquid→ low fiber
- Plan for safe discharge pending above
Patient education:
- Educate regarding the importance of completing above steps before discharge, to ensure safety.
- Educate regarding the importance of treating diverticulitis early on to prevent complications such as perforation, abscess and fistulas. Look out for s/s of recurrent diverticulitis such as blood in stool, LLQ pain etc.
- Allow the colon to heal by maintaining a low fiber diet. Once acute attack is resolved, maintain a high fiber diet and hydration to prevent future attacks by promoting regular BM.
- Educate regarding the importance of completing the full course of antibiotics, even if symptoms resolve.
- Follow up with GI.