History
53 year old male with no significant PMHx presented to ED 3 days ago with complaints of rectal pain on defecation. He was diagnosed with perianal abscess. Incision and drainage of the abscess was performed at the bedside by the surgery team. He also had a POC blood sugar level of 328 with an anion gap of 23 (DKA), with newly diagnosed type 2 diabetes mellitus. Pt was admitted to obtain glucose control with an uneventful hospital course.
S
Patient was seen and examined at bedside. Pt denied any pain, but admits to mild discomfort upon defecation. He admits to having normal bowel movements with some streaks of blood on the stool, which he says is still from the abscess. He is also urinating dark yellow urine. Denies nausea and vomiting. He is tolerating a solid food diet and is ambulating.
O
Vitals:
- HR: 90 BPM regular rate, rhythm and amplitude (range: 73-90)
- RR: 17/min, regular rate and rhythm, unlabored (range: 14-23)
- Systolic BP: 156 (range: 146-156)
- Diastolic BP: 87 (range: 87-104)
- Temp: 36.4 C, orally
- Glucose: 255 (range: 111-255)
I/Os:
- Urine: 600/600 pale yellow
Physical exam:
- General: Well developed, obese male in no apparent discomfort. Appears stated age of 53. Alert and oriented x3.
- Lungs: Unlabored breathing, clear to auscultation and percussion bilaterally. No adventitious sounds.
- Heart: Regular rate and rhythm. S1 and S2 are distinct with no murmurs, S3 or S4. No splitting of S2 or friction rubs appreciated.
- Abdomen: Abdomen flat and symmetric with no scars, striae or pulsations noted. Bowel sounds normoactive in all 4 quadrants with no aortic/renal/iliac or femoral bruits. Mild tenderness to palpation and tympanic throughout, no guarding or rebound noted. No hepatosplenomegaly to palpation. No CVA tenderness noted.
- Perirectal: Minimal serosanguinous drainage, minimal induration, minimal tenderness to palpation.
- Extremities: No erythema, warmth or crepitus noted. Non-tender to palpation. Full range of motion of all upper and lower extremities bilaterally.
- Neuro: Sensation is intact bilaterally to pain and light touch. Good muscle tone. Strength is 5/5 bilaterally at the deltoid, biceps, triceps, quadriceps, and hamstrings.
Labs:
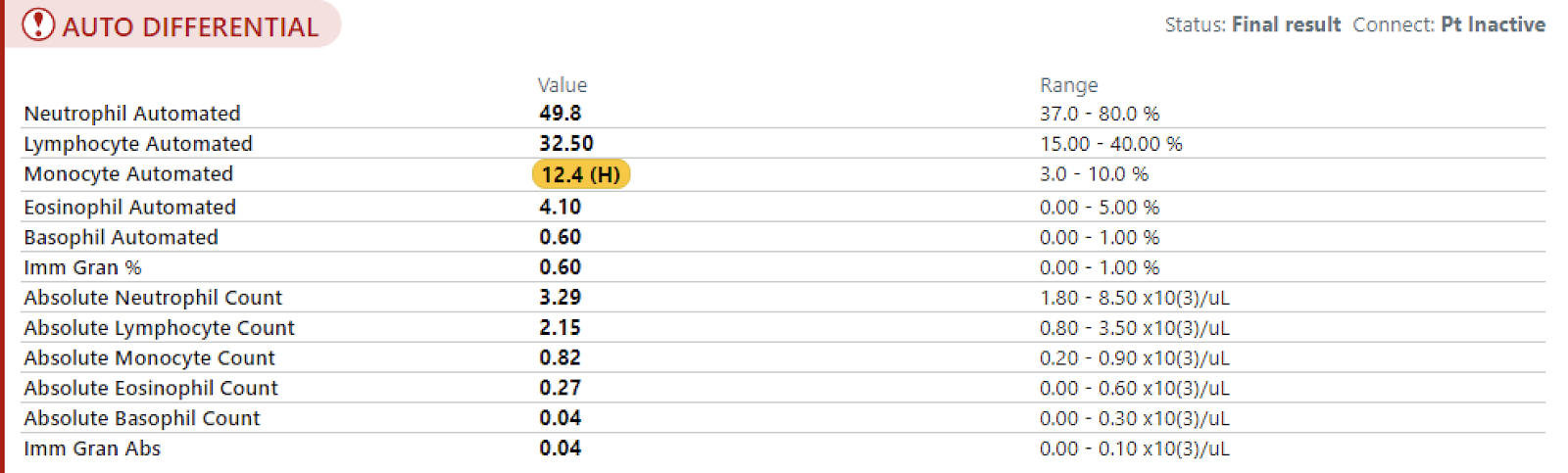
- CBC with diff.

- BMP
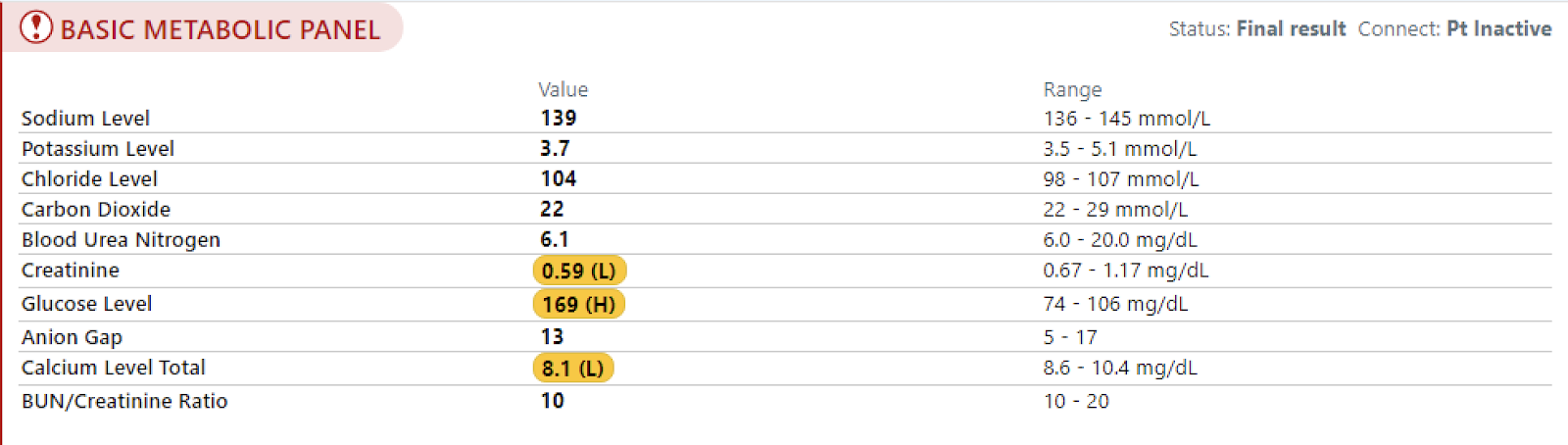
- Glucose

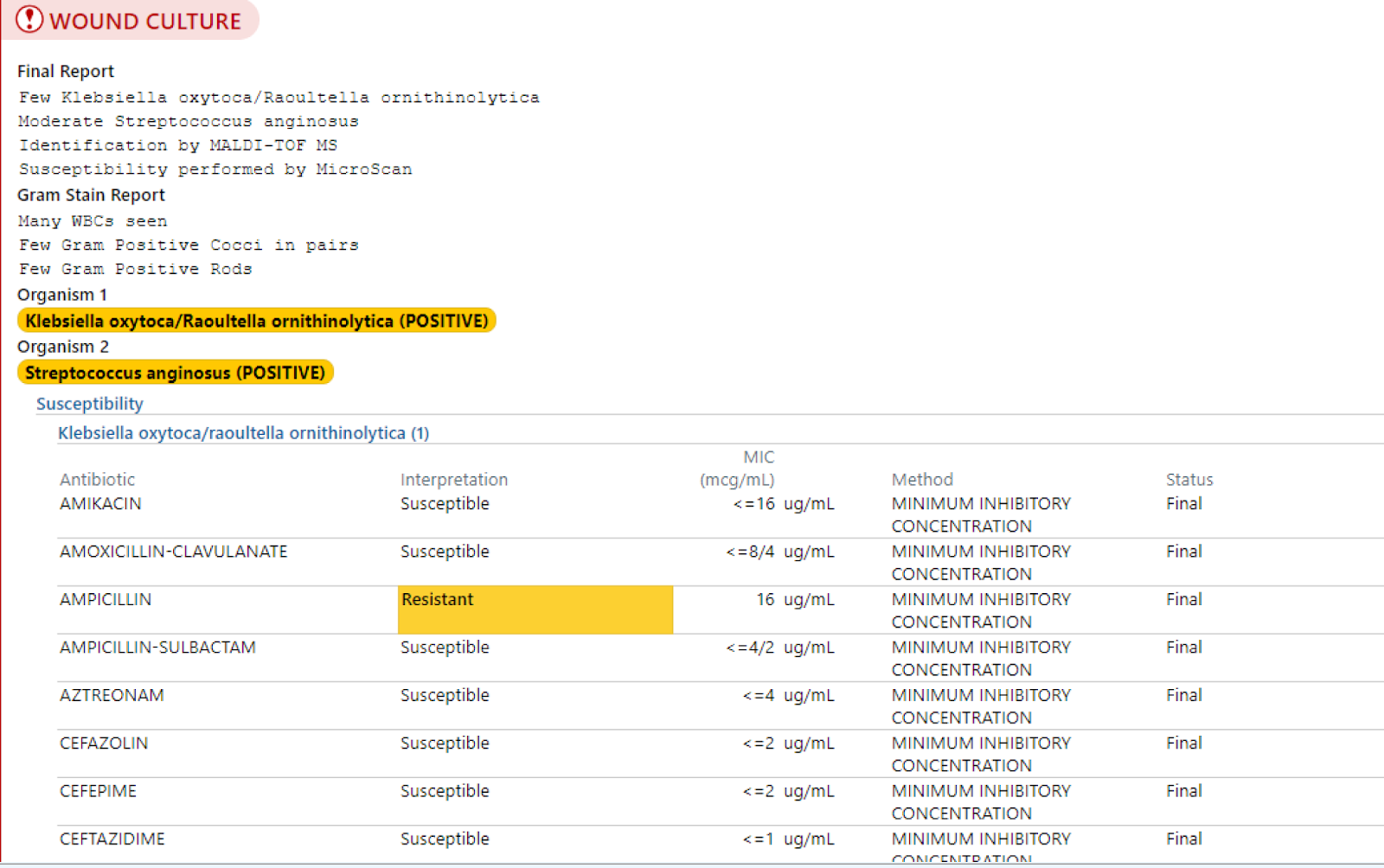
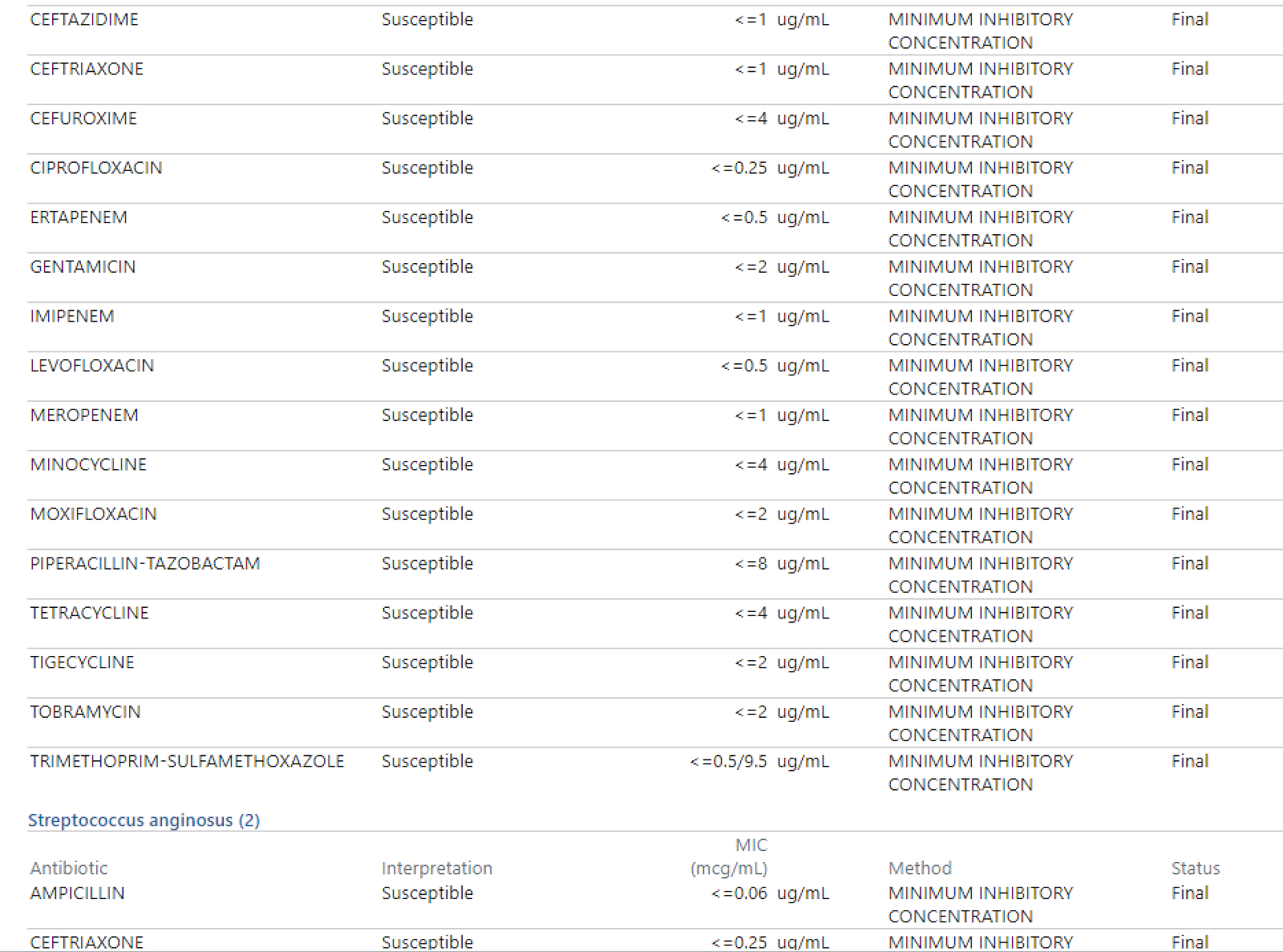
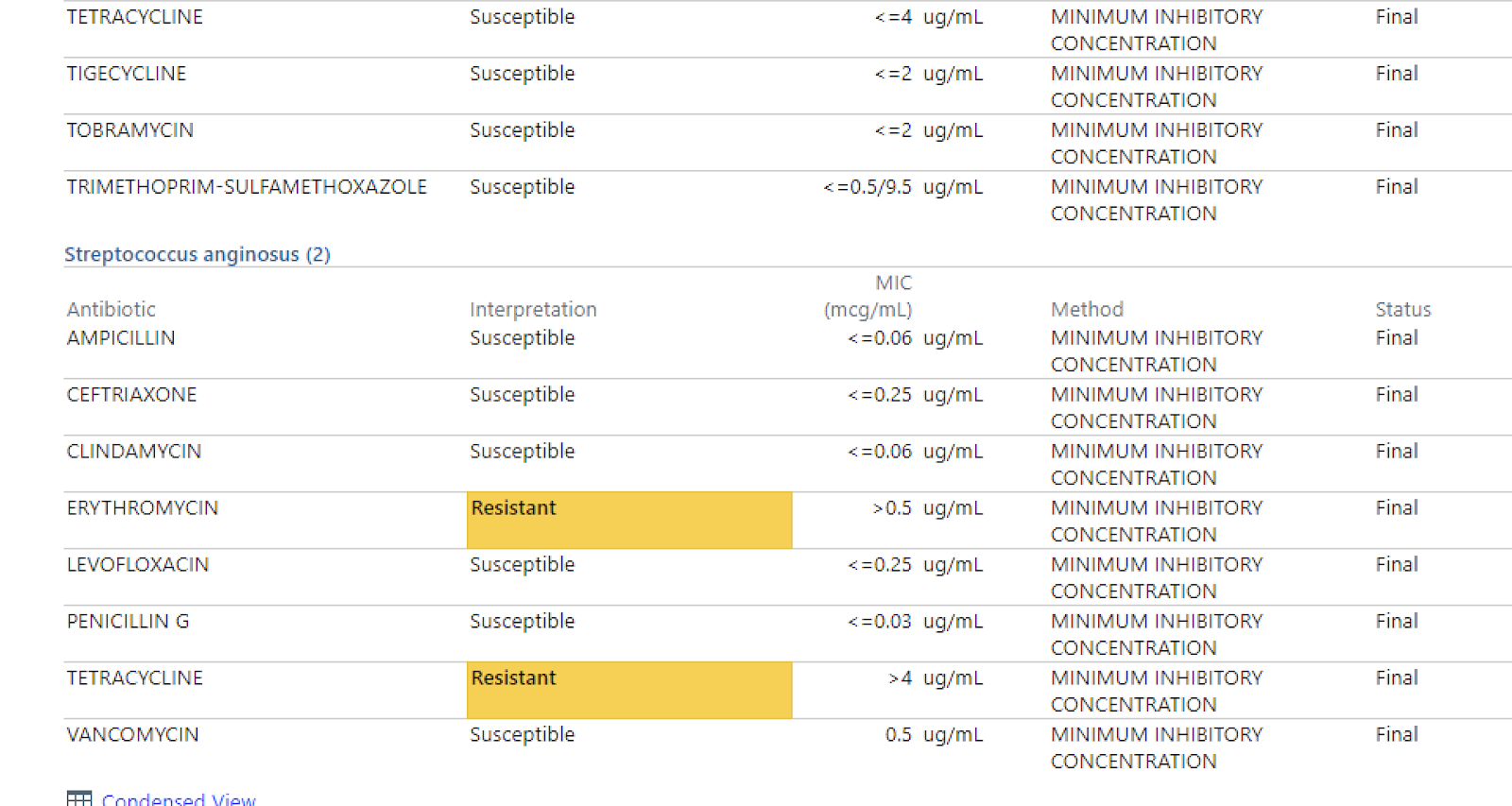
- Wound culture and sensitivity
A
This is a 53 year old male, HD 4 status post bedside incision and drainage of perianal abscess. Pt has been receiving ceftriaxone and metronidazole with good wound healing noted. Pt also had DKA and was able to be weaned off insulin drip. Endo was consulted. Pt is ready for discharge today.
P
Perianal abscess:
- Ciprofloxacin 500 mg PO Q12H x10 days, guided by c/s of the wound and allergy to penicillin
- Metronidazole 500 mg PO TID x10 days
- Acetaminophen 500 mg PO Q6H PRN pain
- Glycolax PO once daily PRN
- Follow up with Dr. Foglia in about 3 weeks
- Return sooner for any worsening fever, chills, bleeding, pain.
- Educate regarding possible pain, limited activity and wound care (hot sitz baths and gauze changes)
Newly diagnosed type 2 diabetes mellitus:
- As per endo- 4 U Insulin Lispro TID before meals + 9 U Insulin Glargine at night
- Nutrition consult
- Education regarding how to administer insulin
- Send Rx for needles, glucometer, test strips, alcohol prep pads
- Follow up with endo and PCP in a week
HTN:
- Losartan as per PCP
- Follow up with PCP in a week