History
CC:
“My stomach is so hard and distended and it really hurts” x 3 days.
HPI:
71 year old with no known pmhx presents to the ED with complaints of abdominal pain and distention x3 days. Pt says the pain is a constant, dull pain that is 10/10 in severity. The pain is diffuse, with no radiation. Pt states the pain came on suddenly and is getting worse over time. Pt says standing up makes the pain feel better, while movement, sitting and lying down makes the pain much worse. Pt also says her stomach looks like “I’m 9 months pregnant and it feels so hard.” Pt notes 1 episode of non-bloody, non-bilious vomiting last night after eating dinner. Pt was able to keep water down this morning. Pt admits to having a soft bowel movement yesterday morning, with no melena or hematochezia noted.
Denies weight loss, fever, chills, fatigue, cough, hemoptysis, dyspnea, chest pain, diarrhea, constipation, previous abdominal surgeries or colonoscopy. Also denies any changes in dietary habits, smoking, alcohol consumption and any recent travel.
Good HPI and relevent ROS
PMHx:
- No known pmhx, surgeries or hospitalizations
Medications:
- No prescription medication use.
- Denies herbal supplement use.
Surgical History:
- No surgical history.
Allergies:
- No known drug/food/environmental allergies
Family History:
- Mother: Deceased, unknown cause at age 80
- Father: Deceased, unknown cause at age 83
- 2 daughters- alive and well
- No known family hx of HTN, diabetes, cancer.
Social History:
- Smoking: Denies
- Alcohol: Denies
- Illicit drug use: Denies past or current use
- Marital History: Widowed
- Language: English
- Occupational History: Retired, previously worked from home as an architect
- Travel: No recent travel
- Home situation: Lives in an apartment in NYC on her own, near her daughters.
- Sleep: Endorses adequate sleep
- Exercise: Walks around the block twice daily
- Diet: Reports balanced diet of lean proteins, carbs, fruits and vegetables
- Caffeine: Denies caffeine use
ROS:
- General: Denies fever, fatigue, chills, night sweats, weight loss/gain, changes in appetite.
- Skin, hair, nails: Denies discolorations, moles, rashes, changes in hair distribution or texture, pruritus.
- HEENT: Denies head trauma, vertigo, visual disturbances, ear pain, hearing loss, tinnitus, epistaxis, discharge, congestion, sore throat, bleeding gums.
- Neck: Denies localized swelling/lumps, stiffness/decreased ROM
- Breast: Denies lumps, nipple discharge, or pain.
- Pulmonary: Denies cough, dyspnea, wheezing, cyanosis, hemoptysis.
- Cardiovascular: Denies chest pain, edema/swelling of ankles or feet, palpitations.
- Gastrointestinal: Admits to abdominal pain, nausea, vomiting and some jaundice. Denies diarrhea, constipation, dysphagia, pyrosis, flatulence, eructation, rectal bleeding, hemorrhoids or blood in stool.
- Genitourinary: Denies urinary frequency, nocturia, dysuria, urgency, flank pain, oliguria, polyuria and incontinence.
- Menstrual/Obstetrical: G2P2002, LMP 2005; not currently sexually active
- Musculoskeletal: Denies back pain, muscle pain, joint pain, arthritis and joint swelling.
- Nervous system: Denies seizures, headache, loss of consciousness, sensory disturbances, ataxia, loss of strength, change in cognition/mental status/memory.
- Peripheral vascular: Denies intermittent claudication, coldness or trophic changes, varicose veins, peripheral edema, or color changes.
- Hematologic: Denies anemia, easy bruising or bleeding, lymph node enlargement, history of DVT/PE.
- Endocrine: Denies polyuria, polydipsia, polyphagia, heat or cold intolerance, goiter, excessive sweating, or hirsutism.
- Psychiatric: Denies feelings of helplessness, hopelessness, lack of interest in usual activities, or suicidal ideations, anxiety, obsessive/compulsive disorder, or ever seeing a mental health professional.
Physical
General:
- Well developed, well-nourished female in some discomfort, unable to find a comfortable position lying down. Appears stated age of 71. Neatly groomed, alert and oriented x3.
Vital Signs:
- BP: 96/68 mm Hg
- RR: 19/min, regular rate and rhythm, unlabored
- P: 86 beats per minute, regular rate, rhythm and amplitude
- T: 97.7 degrees F (oral)
- O2 Sat : 100% room air
- Height: 67 inches Weight: 127 lbs BMI: 19.9
Skin & Head:
- Skin: Warm and moist, good turgor. Nonicteric, no lesions, scars, or tattoos noted. Slight jaundice throughout her body.
- Eyes: Symmetrical OU. No strabismus, exophthalmos, or ptosis. Sclera white, no icterus noted, cornea clear, conjunctiva pale.
- Mouth: Dry, pale mucosa. No cyanosis. No masses, lesions, leukoplakia. Good dentition. No obvious dental caries noted. No deviation of the tongue.
Thorax and Lungs:
- Chest: Symmetrical, no deformities, no trauma. Respirations unlabored/ no paradoxical respirations or use of accessory muscles noted. Non-tender to palpation throughout.
- Lungs: Clear to auscultation and percussion bilaterally. No adventitious sounds.
Cardiac Exam:
- Heart: Regular rate and rhythm. S1 and S2 are distinct with no murmurs, S3 or S4. No splitting of S2 or friction rubs appreciated.
Abdominal Exam:
- Abdomen severely distended and hard with no scars, striae or pulsations noted. No bowel sounds appreciated in any quadrants. Mildly tender to palpation with no guarding or rebound noted. No CVA tenderness appreciated.
Mental status exam:
- Patient is well appearing, has good hygiene and is neatly groomed. Patient is alert and oriented to name, date, time and location. Speech and language ability intact, with normal quantity, fluency, and articulation. Patient denies changes to mood. Conversation progresses logically. Insight, judgment, cognition, memory and attention intact.
Peripheral Vascular System:
- Extremities are warm and without edema. No varicosities or stasis changes. Calves are supple and nontender.
Differential diagnosis:
- Volvulus
- This pt has multiple findings consistent with this diagnosis. Volvulus is the twisting of the intestine on itself. It presents as sudden onset of abdominal pain, distention, nausea, vomiting and abdominal tenderness. These are all present in this patient. Additionally, the patient had no bowel sounds, a common finding in volvulus. A risk factor for volvulus is being over the age of 65, as this pt is.
- Small bowel obstruction
- This pt presents with abdominal pain and distention, common finding with small bowel obstruction. Additionally, the nausea and vomiting suggests this as the diagnosis. Similar to volvulus, being over 65 is a risk factor. However, the greatest risk factor is prior abdominal surgeries, which is not present in this patient. This is why I chose to include this as the second differential.
- Pancreatitis
- Pancreatitis does also present with abdominal pain which is what made me think of this as a differential. Additionally, in later stages it can cause abdominal distention and jaundice. Pancreatitis can also cause nausea and vomiting. This diagnosis is less likely than the above 2 for a few reasons. Firstly, the pain typically radiates to the back which is not a feature in this patient. Also, this patient does not have fever, a typical sign with pancreatitis. Also the biggest cause of pancreatitis is gallstones (which the pt does not have any history of) and alcohol consumption (which this patient denies).
- Hepatic failure with ascites
- The slight yellow discoloration of this patient made me think of hepatic failure, which can lead to ascites. Therefore, the fact that the patient has abdominal distention may be attributed to ascites. However, this is not so likely because the abdomen is hard on palpation and no fluid wave is noted. Another reason why this diagnosis is not so likely is because the patient does not have any known risk for hepatic failure such as alcohol abuse or hepatitis.
- Colorectal cancer
- Colorectal cancer is a cancer that is typically diagnosed in older adults and therefore this pt’s age made me think of this diagnosis. Additionally, later in the course of the disease there may be abdominal pain and distention, due to the obstruction from the tumor. Also this patient denied having any screenings done, including colonoscopy. This diagnosis is lowest on my list because of the acute onset this patient experienced, which is not usual for colorectal cancer. She also denied changes to bowel habits which is a typical symptom of colorectal cancer.
Great pertinent DDx
Labs:
- CBC with diff.

- Type and screen
- A positive
- Coag studies
- aPTT= 27 (reference= 25.1-36.5 seconds)
- PT= 14.1 (reference= 9.4-12.5 seconds)
- INR= 1.2 (reference= 0.9-1.1 ratio)
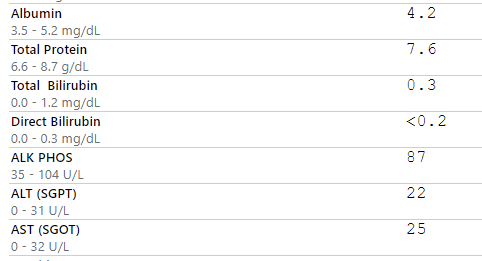
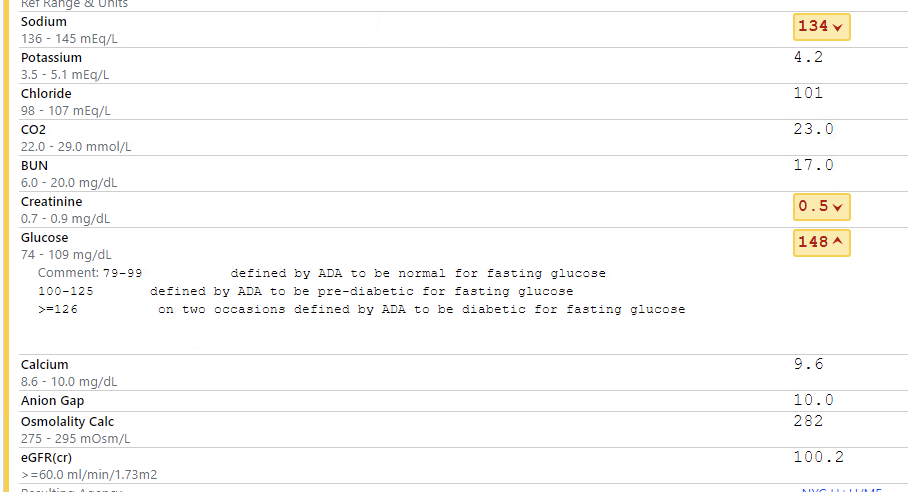
- CMP
- Lipase
- 29 (reference= 13-60 U/L)
Imaging:
- Bedside ultrasound
- No free fluid noted
- Bedside chest and abdominal x-ray
- Markedly dilated air-filled upper abdominal bowel loops consistent with obstruction. There is a 265 mm x 164 mm mid-abdominal distended viscus filled with ingested material or bowel contents. It may be the stomach or a closed loop obstruction of the bowel.
- CT abdomen/pelvis with contrast
- There are massively dilated air-filled bowel loops proximal to a massively distended stool-filled cecal volvulus. There is a large quantity of free intraperitoneal air.
Assessment
- 71 year old with no known pmhx presents to the ED with complaints of abdominal pain and distention x3 days. Pt also experienced one episode of vomiting after eating yesterday. Her last bowel movement was yesterday. On exam, pt has a hard, tender, significantly distended abdomen. There is also notable jaundice of the pt’s skin and dryness of the mucus membranes. All other parts of the exam are within normal limits. Labs are significant for low RBC count (3.68) with associated decreased hgb and hct. Additionally, pt has increased PT and INR. On CT a large cecal volvulus is noted with suspected perforation.
Diagnosis:
- Cecal volvulus with perforation
Plan
- Perforation:
- 4.5 g piperacillin-tazobactam in 100 mL D5W Q6H
- Pain control:
- IV acetaminophen 1,000 mg
- IV ketorolac injection 15 mg
- If no proper pain relief attained→ 2 mg morphine push dose
- Anti-emetic:
- IV ondansetron injection 4 mg
- Dehydration:
- IV infusion normal saline 1,000 mL
- Surgical consult for likely surgical intervention
- NPO
Excellent management to obtain CXR with abdominal XR while pending CT imaging, this drastically improves morbidity and mortality rates by allowing you to have early surgical intervention if patient started to become increasingly hypotensive while pending CT imaging. Patient may be brought directly to OR w/ diagnosis in hand. Good coverage w/ antibiotics, would have avoided ketorolac in likely ex-lap patient and preferred opiates for pain control.
Should have presented this case!