History
76 year old female with PMHx of diverticulosis and COPD and PSHx of L hemicolectomy with end transverse colostomy in October of 2023 presented to ED 3 days ago due to dark red blood quickly filling her colostomy bag. Pt was admitted and over the course of her stay she had CT, endoscopy and colonoscopy which were all unable to locate the source of the bleed. Pt has been hemodynamically unstable and has been requiring frequent transfusions of pRBCs.
#2: S
Pt was seen and examined at bedside. Pt says there is still bloody output in her colostomy bag. She also says her mouth is very dry and eating cups of ice makes it much better. Over the night pt states she has experienced nausea for which she was given ondansetron, pantoprazole and maalox which helped. She no longer feels the nausea. Pt received 2 U of pRBC overnight and has had no negative reactions to them. Pt denies pain, nausea, vomiting, dyspnea, chest pain, lightheadedness and numbness. Pt has not been ambulating.
O
Overnight pt received 2 U pRBC due to falling Hb with no adverse reactions. Pt also underwent NM scan with results attached below. Pt also underwent capsule endoscopy with results pending.
Vitals:
- Temperature: 36.6
- Systolic BP: 101 (range: 97-114)
- Diastolic BP 65 (range: 54-66)
- HR: 102 tachycardic, regular rhythm and amplitude (range: 88-122)
- RR: 18/min, regular rate and rhythm, slightly labored (range: 18-20)
I/Os:
- Urine premafit: 300 dark yellow urine overnight (not recorded during the day)
- Colostomy bag: 350/950 bloody, loose, clotting
Physical exam:
- General: Well developed, well nourished female in no apparent discomfort. Appears stated age of 76. Alert and oriented x3.
- Skin: Warm and moist, good turgor. Nonicteric, no lesions, scars, or tattoos noted. No pallor.
- Lungs: Slightly labored breathing, clear to auscultation and percussion bilaterally. No adventitious sounds.
- Heart: Regular rate and rhythm. S1 and S2 are distinct with no murmurs, S3 or S4. No splitting of S2 or friction rubs appreciated.
- Abdomen: Abdomen flat and symmetric. Colostomy bag in place with dark red, clotting blood. No other scars noted. Bowel sounds normoactive in all 4 quadrants with no aortic/renal/iliac or femoral bruits. No tenderness to palpation and tympanic throughout, no guarding or rebound noted. No hepatosplenomegaly to palpation. No CVA tenderness noted.
- Neuro: Sensation is intact bilaterally to pain and light touch.
Labs/imaging:
- CT, endoscopy and colonoscopy did not locate the source of bleed and was done earlier in pts hospital stay.
- Results of capsule endoscopy pending.
- NM scan- tagged RBC

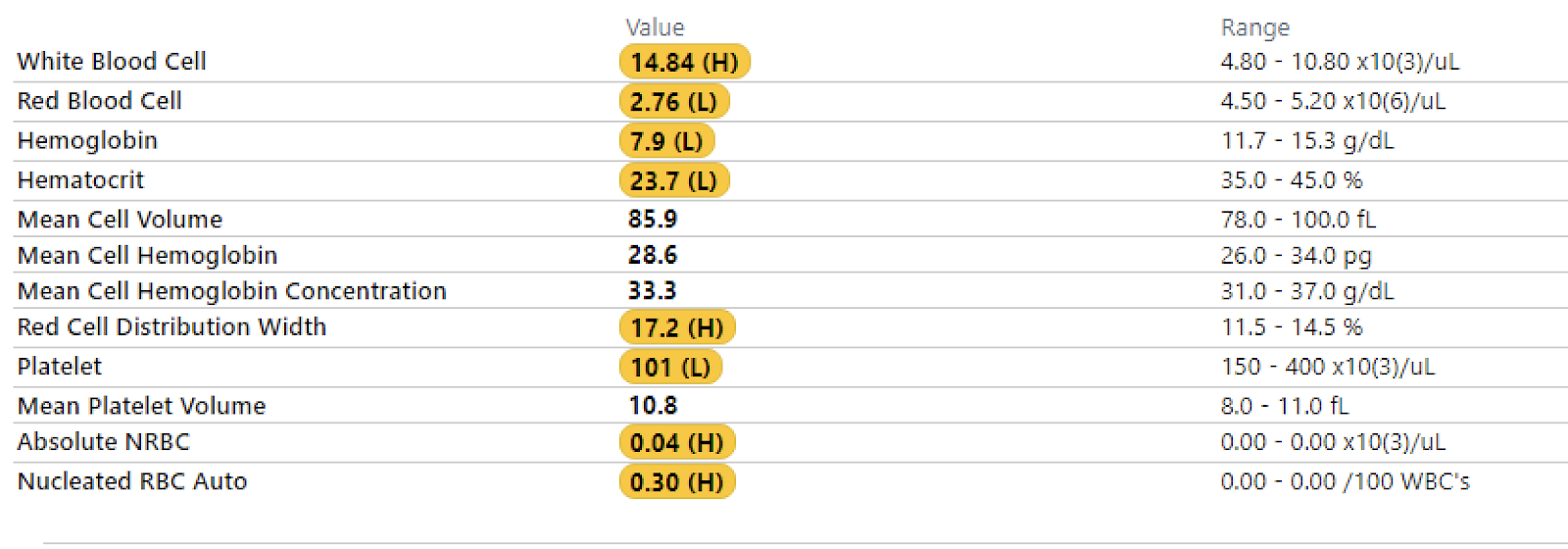
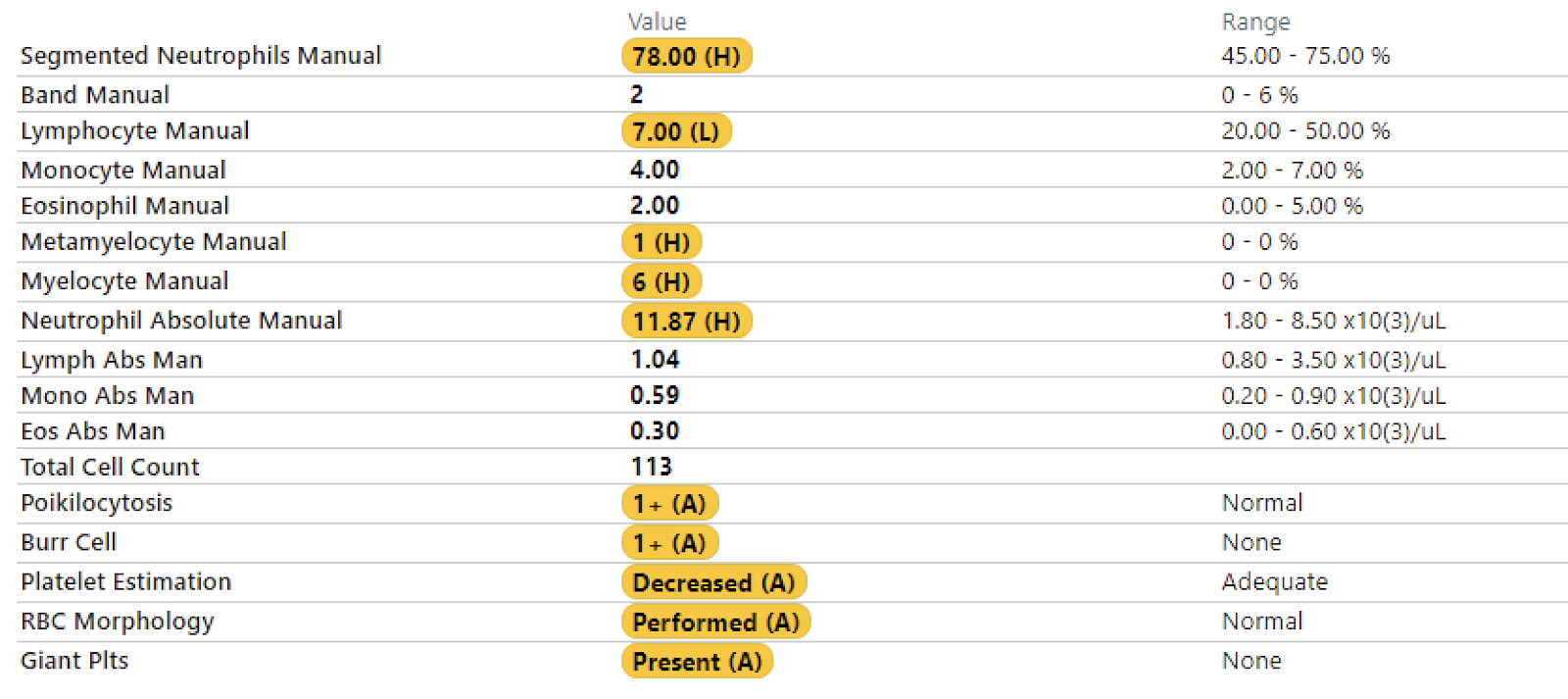
- CBC with diff.
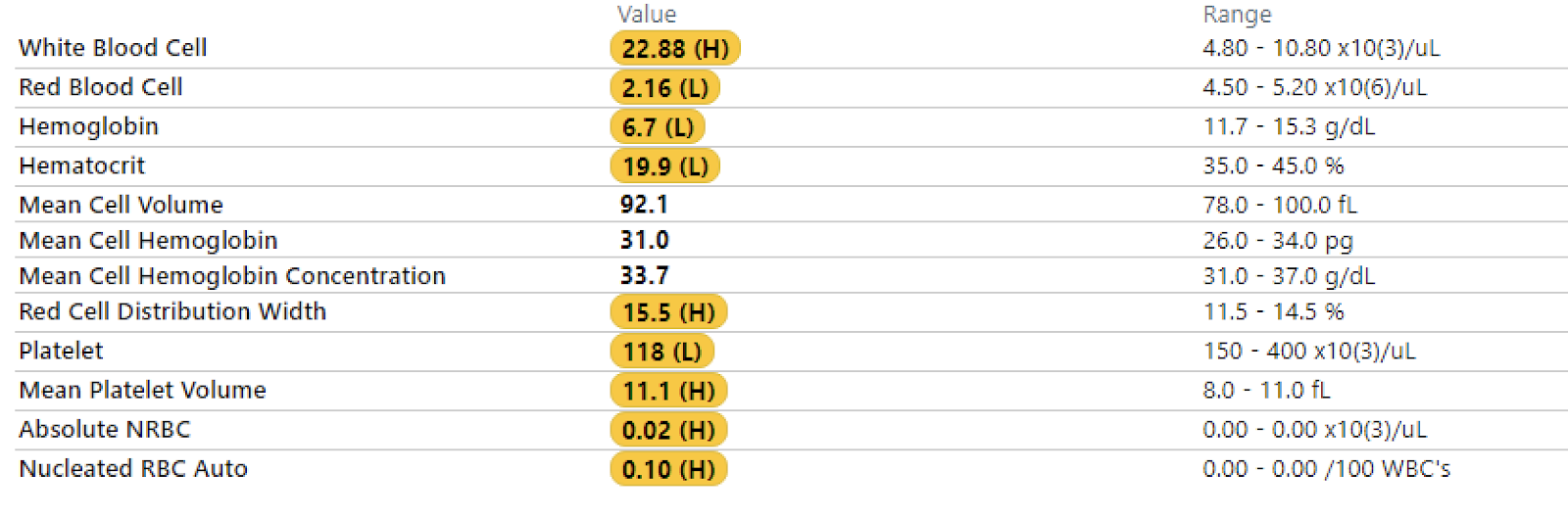
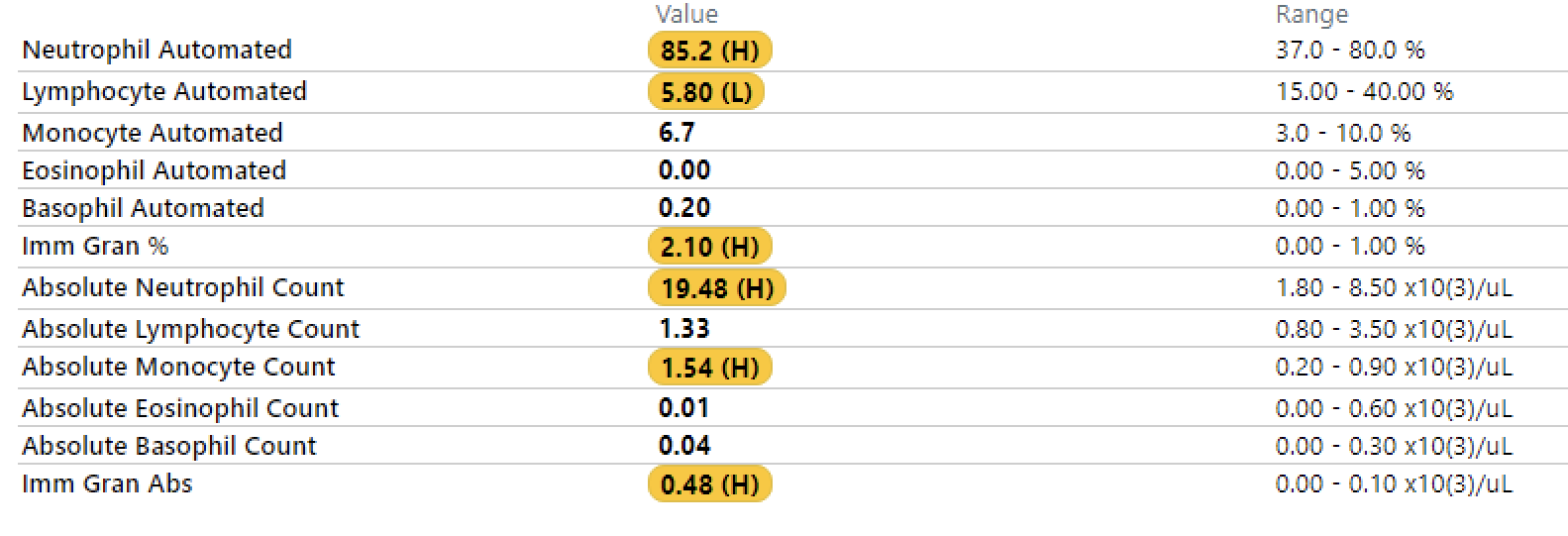
A
This is a 76 year old female, hospital day 5, with PMHx of COPD and diverticulosis and PSHx of L hemicolectomy with end transverse colostomy who has continuous GI bleed of unlocalized source. Pt is in no apparent distress and remains stable with transfusions, 2 U of pRBCs overnight. There is continuous bloody output in her colostomy bag. Currently waiting for the results of the capsule endoscopy.
P
- Await results for further management plan, follow with GI for capsule results
- Post transfusion CBC with serial CBCs (Q4H), transfuse pRBCs PRN
- Follow colostomy output
- Remain NPO
- Keep active T&S
- Tentative operative plans for R hemicolectomy with end ileostomy for persistent bleeding
#3: S
Pt seen and examined at bedside. Pt states that she feels the same as she did yesterday, with continuous blood output in her colostomy bag. She denies pain, nausea, vomiting, dyspnea, chest pain, lightheadedness and numbness.
O
Overnight pt received 2 U pRBC (9 U total since beginning of her hospitalization). Results of capsule endoscopy came back saying that a tiny AVM was noted, but no active bleed was seen. Capsule was retained in the ileum.
Vitals:
- Temperature: 36.4
- Systolic BP: 118 (range: 94-118)
- Diastolic BP 66 (range: 54-66)
- HR: 101 tachycardic, regular rhythm and amplitude (range: 89-118)
- RR: 18/min, regular rate and rhythm, slightly labored (range: 18-20)
I/Os:
- Urine premafit: 600 clear yellow overnight, not recorded during the day
- Colostomy bag: 190/390 dark red, bloody, clotting
Physical exam:
- General: Well developed, well nourished female in no apparent discomfort. Appears stated age of 76. Alert and oriented x3.
- Skin: Warm and moist, good turgor. Nonicteric, no lesions, scars, or tattoos noted. No pallor.
- Lungs: Slightly labored breathing, clear to auscultation and percussion bilaterally. No adventitious sounds.
- Heart: Regular rate and rhythm. S1 and S2 are distinct with no murmurs, S3 or S4. No splitting of S2 or friction rubs appreciated.
- Abdomen: Abdomen flat and symmetric. Colostomy bag in place with dark red, clotting blood. No other scars noted. Bowel sounds normoactive in all 4 quadrants with no aortic/renal/iliac or femoral bruits. No tenderness to palpation and tympanic throughout, no guarding or rebound noted. No hepatosplenomegaly to palpation. No CVA tenderness noted.
- Neuro: Sensation is intact bilaterally to pain and light touch.
Labs/imaging:
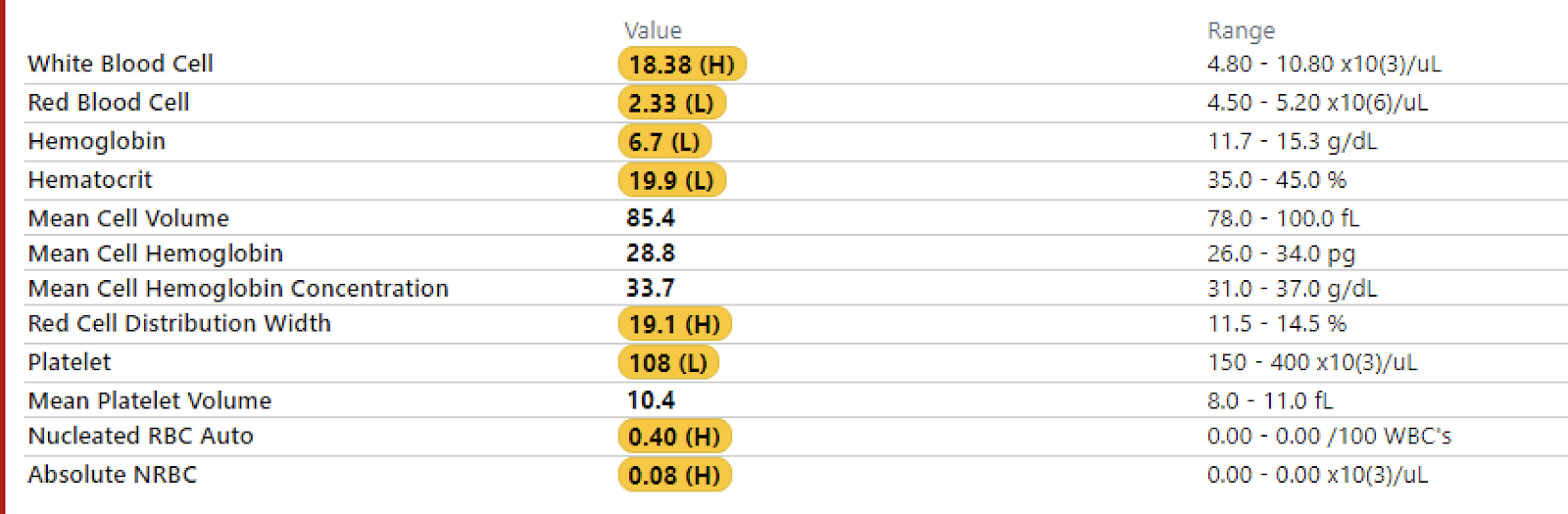
- CBC w/o diff.
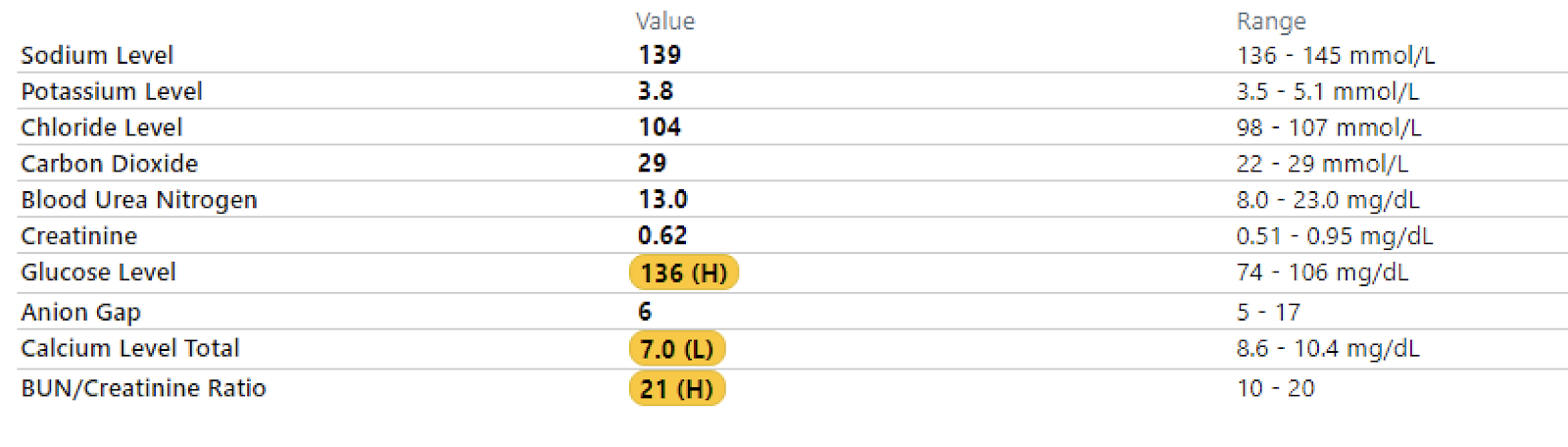
- BMP
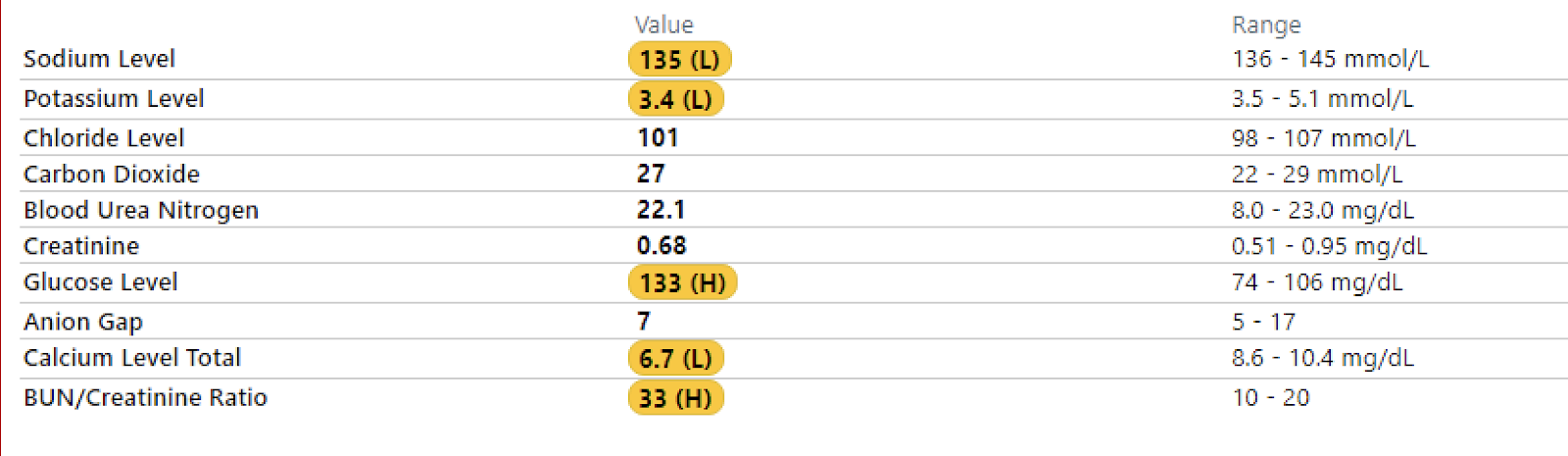
- GFR
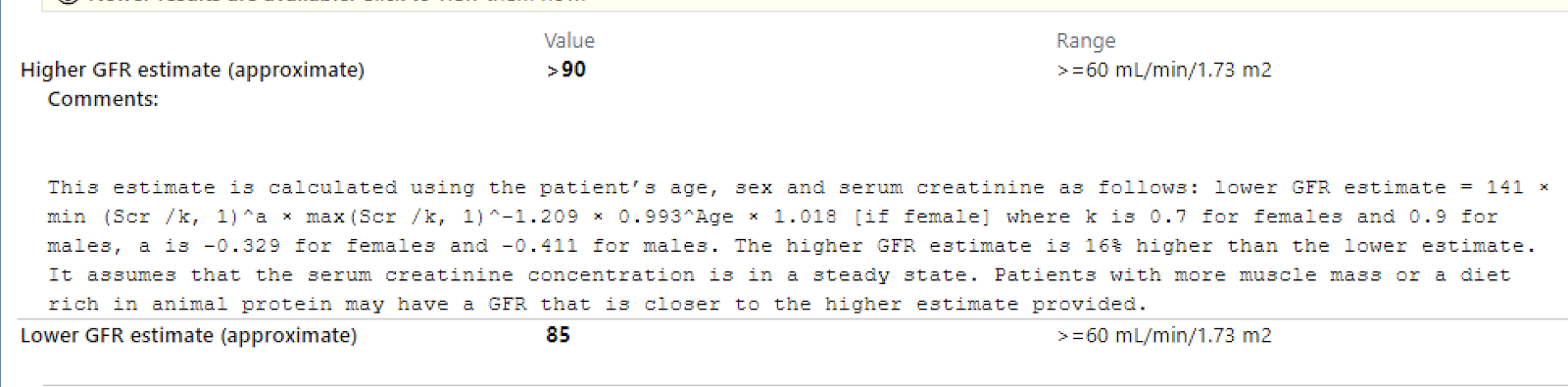
A
76 year old female with an unlocalized lower GI bleed. Pt is continuing to lose blood in her ostomy bag. Hb levels keep dropping, requiring frequent transfusions of pRBC. Prepare for R hemicolectomy.
P
- Obtain all preop labs (CBC, T&S, Coags, kidney functions)
- Consult pulm for operative clearance due to history of COPD
- Continue medications for pain and nausea PRN
- Serial CBCs, transfuse PRN
#4: S
Pt was seen and examined at bedside. Pt states that she feels the same as she did yesterday, with continuous blood output in her colostomy bag. She denies current pain, nausea, vomiting, dyspnea, chest pain, lightheadedness and numbness. Pt does say that she felt nauseous from the golytely and therefore she did not finish it. The overnight nurse confirms this and says that the pt only drank about half of the golytely.
O
Overnight pt received 2 U pRBC (11 U total since beginning of her hospitalization).
Vitals:
- Temperature: 37
- Systolic BP: 114 (range: 90-114)
- Diastolic BP 69 (range: 55-69)
- HR: 102 tachycardic, regular rhythm and amplitude (range: 89-110)
- RR: 16/min, regular rate and rhythm, slightly labored (range: 16-20)
I/Os:
- Urine premafit: 600 clear yellow overnight, not recorded during the day
- Colostomy bag: 800/1100 dark red, bloody, clotting
Physical exam:
- General: Well developed, well nourished female in no apparent discomfort. Appears stated age of 76. Alert and oriented x3.
- Skin: Warm and moist, good turgor. Nonicteric, no lesions, scars, or tattoos noted. Slight pallor.
- Lungs: Slightly labored breathing, clear to auscultation and percussion bilaterally. No adventitious sounds.
- Heart: Regular rate and rhythm. S1 and S2 are distinct with no murmurs, S3 or S4. No splitting of S2 or friction rubs appreciated.
- Abdomen: Abdomen flat and symmetric. Colostomy bag in place with dark red, clotting blood. No other scars noted. Bowel sounds normoactive in all 4 quadrants with no aortic/renal/iliac or femoral bruits. No tenderness to palpation and tympanic throughout, no guarding or rebound noted. No hepatosplenomegaly to palpation. No CVA tenderness noted.
- Neuro: Sensation is intact bilaterally to pain and light touch.
Labs/imaging:
- CBC w/ diff.
- BMP
- T&S

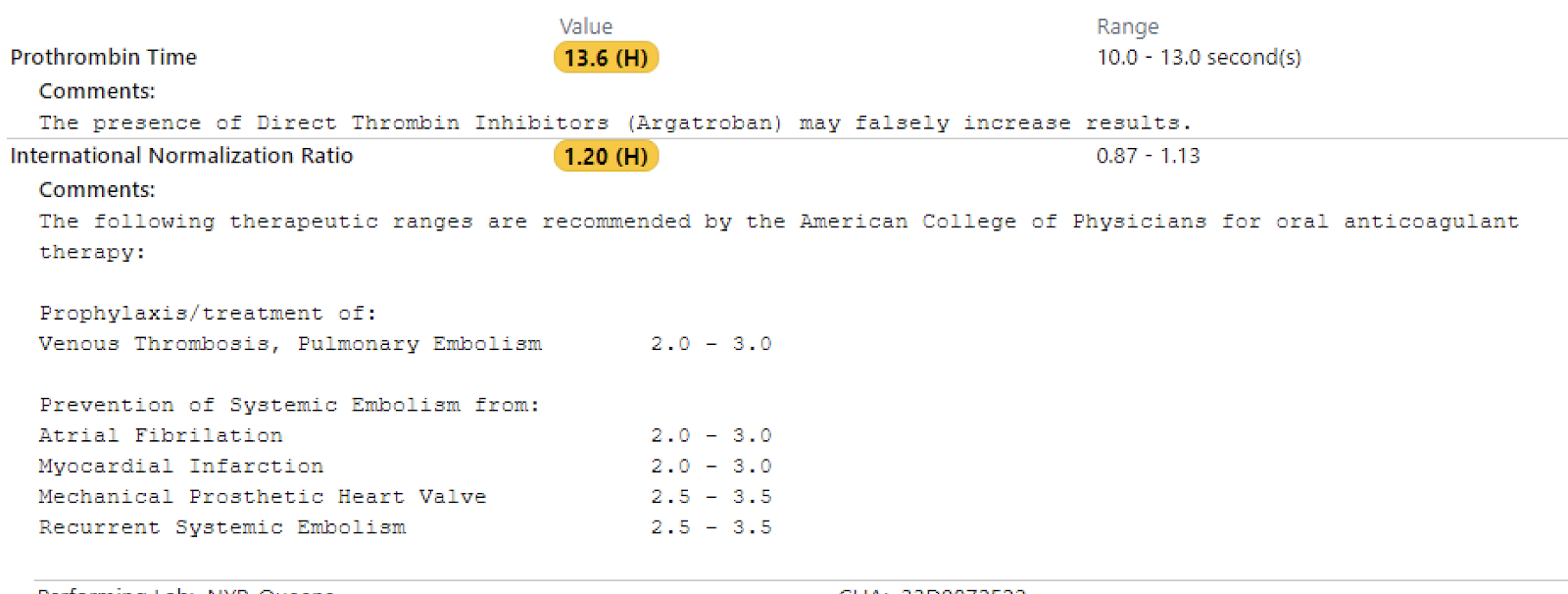
- PT/INR
A
76 year old female with lower GI bleed of unlocalized source. Pt remains needing transfusions. Clearance for surgery obtained and pt is ready for the OR.
P
- R hemicolectomy with end ileostomy scheduled for today
- Monitor progress post surgery