History
CC:
“Those surgeons are not managing my pain after surgery” x3 days.
HPI:
Pt is a 74 year old male with pmhx of HLD, ulcerative colitis, chronic diarrhea, DVT/PE presents to ED for abdominal pain. Pt’s surgical history is significant for total proctocolectomy and a later ileal pouch-anal anastomosis. Pt was recently admitted to NSUH from 9/12 to 9/15 for exploratory laparotomy, lysis of adhesions and revision of prior small bowel anastomosis due to obstruction. Today pt comes in for abdominal pain that has been persisting since this most recent surgery. Pt states that after his surgery on 9/12, he had been requiring oxycodone 10 mg Q4H. His pain was much improved, and he was able to ambulate without issue on the day of discharge. He was discharged with oxycodone 5mg Q6H x 8 tabs which he ran out of within a day. He called his surgeon’s office who gave him additional oxycodone 5 mg tabs but he ran out of this too. Surgeon then refused to give him more oxycodone.
Pt now states that the abdominal pain is mainly located around the incision site, located at the umbilicus, but does spread to his whole abdomen. He says that the pain is constantly there, however it is milder in severity, about 4/10 when lying down. When he walks around, the pain is a sharp 10/10 pain. Pt has associated nausea, which has induced a loss of appetite. Pt says BM have been unchanged since baseline, experiencing small burden, frequent BM for which he takes opium tincture. Pt maintains angry affect stating he requires extreme pain control including opioids due to his constant use of pain medications and his high tolerance.
Denies vomiting, fever, chills, dyspnea, dysuria, urinary frequency, melena/hematochezia, constipation and diarrhea.
Pmhx:
- HLD
- Ulcerative colitis
- Chronic diarrhea
- DVT/PE
Home medications:
- Atorvastatin 10 mg PO 1 tab once a day at bedtime for HLD
- Ondansetron 4 mg PO 1 tab Q6H PRN nausea
- Opium Tincture PO 0.6 mL 4 times a day as directed by GI for chronic diarrhea
- Xarelto 20 mg PO 1 tab once a day for hx of PE/DVT
- Acetaminophen 325 mg PO 2 tabs Q6H PRN pain
- Oxycodone 5 mg PO 1 tab Q6H PRN severe pain
Hospital medications:
- IV acetaminophen 1,000 mg x1 in ED
- IV morphine 4 mg x1 in ED
- IV ondansetron 4 mg Q8H PRN nausea/vomiting
- PO Opium tincture 6 mg 4 times a day
Surgical History:
- Total proctocolectomy- 2012 due to ulcerative colitis, no known complications
- Ileal pouch-anal anastomosis- 2013, with resulting chronic diarrhea and SBO
- Exploratory laparotomy, lysis of adhesions and revision of prior small bowel anastomosis- 9/12/24
Allergies:
- No known drug/food/environmental allergies
Family History:
- Father- deceased, unknown age, hx of lung cancer dx at unknown age
- No known family hx HTN, DM, cardiovascular disease
Social History:
- Smoking: Denies
- Alcohol: Denies
- Illicit drug use: Denies
- Marital History: Married
- Language: English
- Occupational History: Retired
- Travel: No recent travel
- Home situation: Lives with wife on long island, kids no longer live at home, but live nearby.
- Sleep: Endorses sleeping about 7-9 hours at night and feeling well rested
- Exercise: Typically takes walks with his wife, but due to pain he cannot walk.
- Diet: Admits to a diet balanced with proteins, carbs and vegetables. But admits to loss of appetites due to nausea.
- Caffeine: Denies
ROS:
- General: Admits to loss of appetite. Denies night sweats, chills, weight loss/gain, fever and fatigue.
- Skin, hair, nails: Denies discolorations, moles, rashes, changes in hair distribution or texture, pruritus.
- HEENT: Denies head trauma, vertigo, visual disturbances, ear pain, hearing loss, tinnitus, epistaxis, discharge, congestion, sore throat, bleeding gums.
- Neck: Denies localized swelling/lumps, stiffness/decreased ROM
- Pulmonary: Denies dyspnea, cough, wheezing, cyanosis and hemoptysis.
- Cardiovascular: Denies palpitations, chest pain and swelling of lower extremities.
- Gastrointestinal: Admits to abdominal pain, nausea and typical diarrhea. Denies constipation, dysphagia, pyrosis, flatulence, eructation, rectal bleeding, hemorrhoids, blood in stool, vomiting and bloating..
- Genitourinary: Denies urinary frequency, nocturia, dysuria, urgency, flank pain, oliguria, polyuria and incontinence.
- Musculoskeletal: Denies joint pain, joint swelling, back pain, muscle pain and arthritis.
- Nervous system: Denies seizures, headache, loss of consciousness, ataxia, loss of strength, change in cognition/mental status/memory.
- Peripheral vascular: Denies intermittent claudication, coldness or trophic changes, varicose veins, peripheral edema, or color changes.
- Hematologic: Denies anemia, easy bruising or bleeding, lymph node enlargement, history of DVT/PE.
- Endocrine: Denies diaphoresis, polyuria, polydipsia, polyphagia, heat or cold intolerance, goiter or hirsutism.
- Psychiatric: Denies feelings of helplessness, hopelessness, lack of interest in usual activities, or suicidal ideations, anxiety, obsessive/compulsive disorder, aditory/visual/tactile hallucinations or ever seeing a mental health professional.
Physical
General:
- Well developed, well nourished male in mild apparent discomfort appears stated age of 74. Neatly groomed, in hospital gown, alert and oriented x4. Ambulation not witnessed.
Vital Signs:
- BP: 115/65 mm Hg
- R: 19/min, regular rate and rhythm, unlabored
- P: 69 beats per minute, regular rate, rhythm and amplitude
- T: 97.8 degrees F (oral)
- O2 Sat : 99% room air
- Height: 67 inches Weight: 154 lbs BMI: 24.1
Skin & Head:
- Skin: Warm and moist, good turgor. Nonicteric.
Thorax and Lungs:
- Chest: Symmetrical, no deformities, no trauma. Respirations unlabored/ no paradoxical respirations or use of accessory muscles noted. Non-tender to palpation throughout.
- Lungs: Clear to auscultation and percussion bilaterally. No adventitious sounds.
Cardiac Exam:
- Regular rate and rhythm. S1 and S2 are distinct with no murmurs, S3 or S4. No splitting of S2 or friction rubs appreciated.
Abdominal Exam:
- Abdomen with flat contour with no striae or pulsations noted. Bowel sounds normoactive in all 4 quadrants with no aortic/renal/iliac or femoral bruits. Mild tenderness diffusely, no guarding or rebound noted. Incision located by umbilicus is clean, dry and intact with no erythema or pus.
Mental status exam:
- Patient is well appearing, has good hygiene and is neatly groomed. Patient is alert and oriented to name, date, time and location. Speech and language ability intact, with normal quantity, fluency, and articulation. Patient admits to feeling upset with his situation. Conversation progresses logically. Insight, judgment, cognition, memory and attention intact.
Differential diagnosis:
- Post-op abdominal pain
- Drug seeking behavior
- Opioid induced hyperalgesia
- Surgical site infection
- UTI
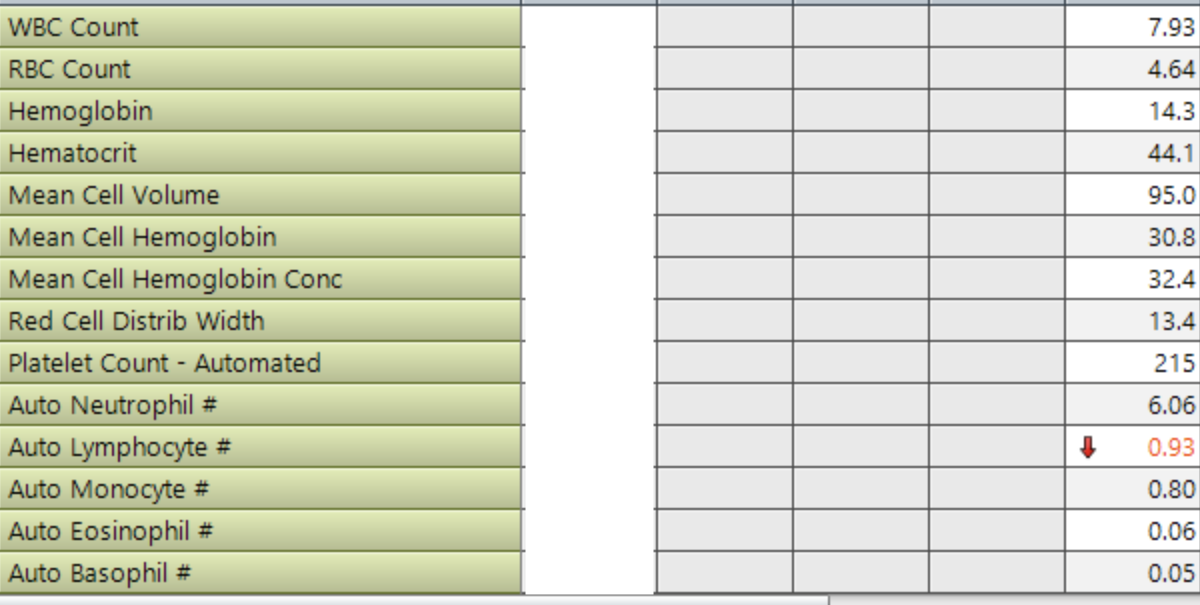
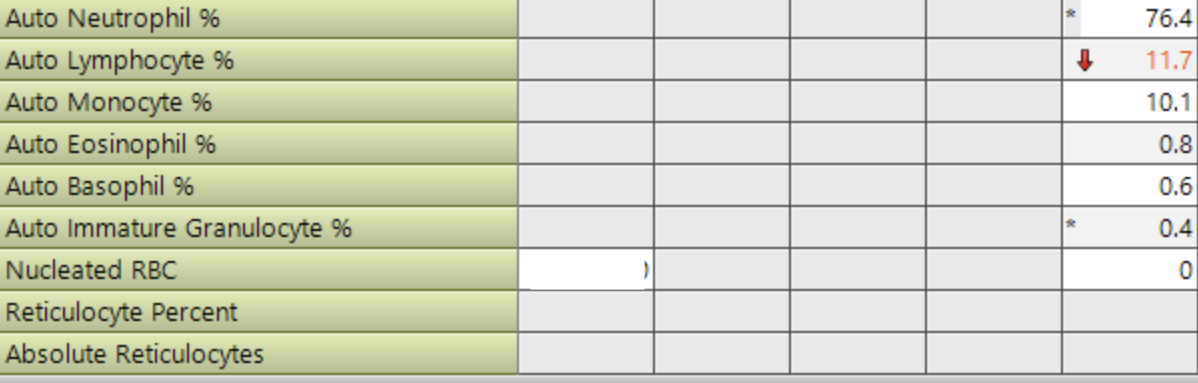
Labs:
- CBC
- CMP
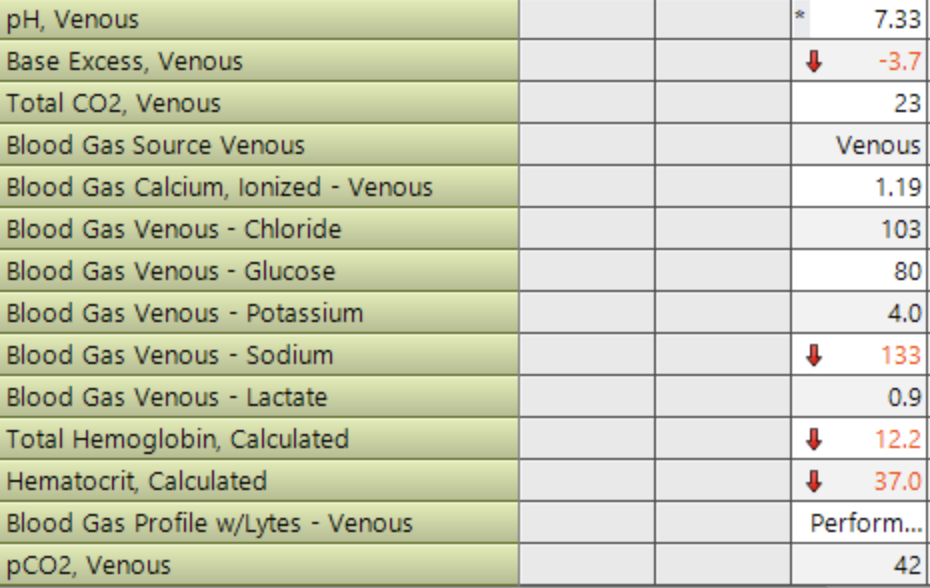
- VBG
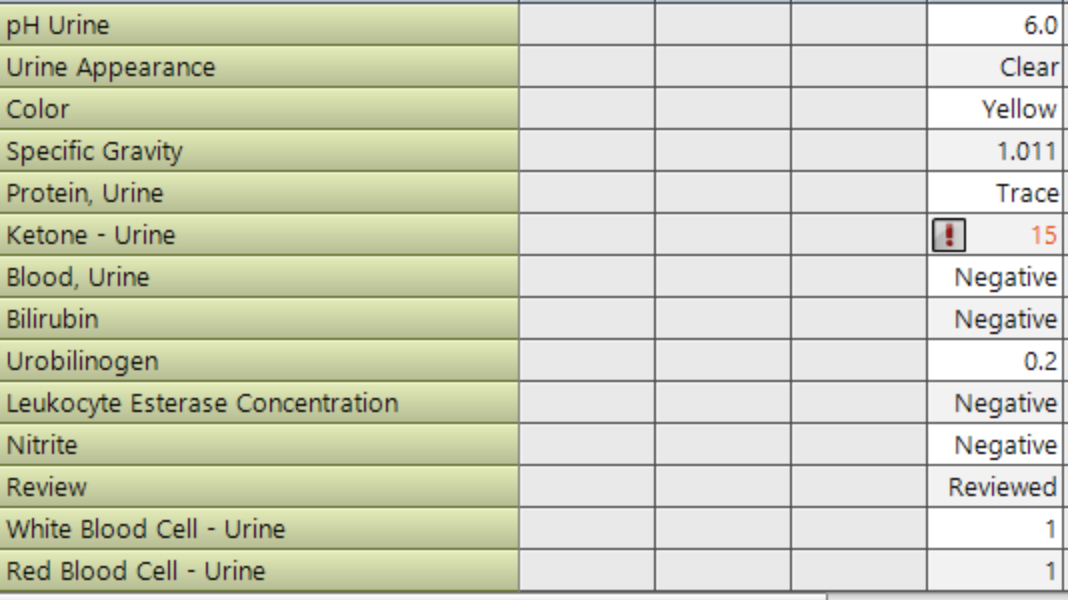
- U/a


Imaging:
- EKG
- Normal sinus rhythm
Assessment:
- 74 year old male with a pertinent past surgical history of total proctocolectomy and IPAA in 2012 and 2013 respectively who is dependent on opium tincture for resultant chronic diarrhea. Surgical history is also significant for recent exploratory laparotomy and lysis of adhesions on 9/12. Pt presents today, 3 days after discharge, with complaints of severe, persistent abdominal pain despite oxycodone prescription. Pt is insistent regarding the need for opioid pain control due to his unique circumstance. On exam, pt appeared to be only mildly uncomfortable with mild diffuse abdominal tenderness. Incision appeared clean and dry. At this time, labs are unremarkable and there are no images to review.
Diagnosis:
- Post-op abdominal pain
Plan:
- Post-op abdominal pain
- General surgery consult
- Consistent with post-op pain. Recommend pain management consult.
- Pain management consult
- Check Istop
- Continue with pain regimen outlined by pain management
- Plan for discharge once pain is stabilized
- General surgery consult
- Chronic diarrhea
- Continue with opium tincture
- HLD
- Continue with atorvastatin
- History of PE/DVT
- Continue with rivaroxaban
Patient education:
- Educate regarding risks of opioid use including tolerance, dependence and addiction. Discuss alternatives to opioid medications including acetaminophen, ibuprofen and physical therapy.
- Instruct on changing the dressing of incision and looking out for infection (erythema, swelling, drainage).
- Encourage gentle movement to help with healing muscles and preventing DVT/PE.
- Return precautions- worsening abdominal pain, fever, signs of infection.
- Set realistic expectations for recovery, including how pain should gradually improve and what normal post-surgical progress looks like.
- Educate pt regarding importance of follow up with surgeons to monitor recovery.
- Provide information about support services, such as pain management specialists, counseling, or patient support groups, if needed.